0.8 What is Project RISE?
Project RISE is a mixed-methods collaborative project aimed at harnessing the power of ritual to improve the efficacy of Accredited Social Health Activists (ASHAs) in Bihar, India. The ASHA role was part of an initiative of the Indian Government’s 2005 National Rural Health Mission (NRHM) intended to improve healthcare in rural areas where services are often lacking.
ASHAs are a type of Community Health Worker (CHW). CHWs are an important force for improving health outcomes (Liu et al. 2011). For good reason, much of the global health community is concerned with finding approaches for improving CHW performance as well as other ways to leverage the embeddedness of CHWs to expand the suite of behaviors that CHWs can positively influence (Smittenaar et al. 2020).
Evaluations of the ASHA program have suggested that the frequency and quality of interactions between ASHAs and beneficiaries can be improved (Lyngdoh et al. 2018; Koehn et al. 2020). However, finding the best ways to optimize CHW performance, and to sustainably improve it, have proved elusive (Scott, George, and Ved 2019).
Project RISE is a novel approach for identifying strategies to improve ASHA motivation and performance. ASHAs are among the most numerous of all CHWs. Bihar alone has about 100 thousand ASHAs and India has nearly one million. The primary health focus of Project RISE is the ASHA’s contribution to perinatal (maternal and newborn) health, but ASHAs are often involved in a variety of health-related initiatives at any given time. For example, they have been instrumental in the frontline response to the COVID-19 pandemic.
Project RISE uses a ritual lens and embraces complexity, which allows for insights into taken-for-granted aspects of ASHA motivation and performance and the development of novel research and design perspectives. Importantly, rituals, defined here as socially stipulated normative behaviors, are not unique to obscure or traditional cultural settings. Rather, they are universal to human cultures and permeate every facet of life in wealthy, educated, and urban settings just as they do in under-resourced, low-education, or rural settings.
0.8.1 Project RISE Central Concepts
Embeddedness -> Liminality
Connectedness + Lived-experience
Project RISE extensively documents and describes the perinatal rituals in Bihar, but many of the benefits of a ritual lens come from the cascading consequences of trying to document and understand what rituals do and how they work
The application of a ritual lens in a study of ASHA motivation identified a series of linked concepts:
As embedded health workers, ASHAs live in the same communities that they serve. The implications of embeddedness for understanding motivation or performance require more exploration. Project RISE identifies unique tensions that emerge as a function of the ASHA’s role as a connector. An emphasis on embeddedness is sometimes what we call the ‘insight hiding in plain sight’ because it is contained in the description of the ASHA role and is common to rationale for CHW programs in general, yet has not been given much attention as a unique source of tension.
As a connector, an ASHA is often at the interface of two groups or communities, without fully belonging to either. This realization pointed us toward the important anthropological concept of liminality. Tensions emerge for health workers who occupy liminal spaces that may be distinct from other roles in the global health community, like doctors or office-oriented officials. This may also identify opportunities for how her position as a local community member might be leveraged more effectively.
Once the importance of liminality becomes apparent, there are operational requirements on the types of data that must be collected in order to understand how liminality affects motivation. In trying to understand liminality, one is immediately faced with a need to understand lived experience. An ASHA’s personal experience as a mother and member of the community shape her approach to the job and her motivation. Differences between ASHAs and beneficiaries shape opportunities, barriers, and messaging for interventions. ASHAs are also mothers and understanding how they draw from their own experiences and perceptions is key to understanding their motivations.
Behaviors, beliefs, and norms do not exist in isolation; they are connected. A ritual lens helps identify this connectivity. Rather than study behaviors in isolation, the RISE approach allows for the identification of constellations of related behaviors and beliefs, and the dynamic nature of how influencers affect maternal health decisions.
Studying ritual facilitates the study of lived-experience and connectivity because ritual is part of the ASHA’s shared experience as members of the same community. Ritual fosters trust and marks transition, and in doing so can alleviate tensions that arise from liminality. ASHAs share knowledge with the women they are meant to provide services to and this in turn can make them effective activists for a health program. Likewise, differences between ASHA and beneficiary lived experience can be as informative as the similarities. These can inform messaging strategies, be used to develop tools for behavior change, and can provide clues for which behaviors are the most resistant to change as well as guidance on connections or barriers to accessing beneficiaries.
Many of the approaches to improving CHW performance have under-performed because they have over-emphasized direct and isolated linkages from incentives (payment systems) to health outcomes and have under-emphasized the importance of community-embeddedness as both a constraint and an opportunity for understanding performance and motivation (Koehn et al. 2020).
In sum, the novel aspects of the Project RISE approach emerge from its central framing on ritual as an essential element of all human cultures that ties together a key aspects of motivation and performance, like trust, group membership, affiliation, habit formation, and status. Most of these elements have been shown by past research on social and behavioral change to be important to fostering successful health initiatives. Unique yet fundamental tensions emerge from being embedded healthworkers in a liminal state and an understanding of the role of ritual can identify pathways for identifying and alleviating those tensions. Once it is clear that a health care worker is often in a liminal state, then it is essential to understand how their lived-experience affects motivation and personal approach to the job. ASHAs are often evaluated for their impact on individual behaviors, which overlooks the fact that behaviors, beliefs, and influencers are connected.
0.8.2 Project RISE Goals
The main objectives of Project RISE include:
To understand the complex cultural ecology of ASHAs, women of reproductive age to whom they connect to the health care system, and other health influencers.
Use this knowledge to devise strategies and solutions for sustainable improvements in the quality of ASHA services by enhancing her motivation and ability.
These objectives are part of the over-arching mission to improve health outcomes in Bihar. In addition, because CHWs are important parts of many rural health care systems, we hope to find general methodological and conceptual tools that can be used by other projects endeavoring to improve health outcomes with similar programs.
To achieve these goals, Project RISE addresses the following:
What: Description of behaviors and rituals that surround pregnancy and childbirth. This includes a description of ritual and health behavior and identifying the ‘target’ behaviors, or those with the greatest potential to positively improve health by intervention.
Who: Understand the sources of information (the influencers) informing decisions to engage or to not engage with perinatal health behaviors
Why: Understanding of the reasoning behind decisions of whether or not to practice these behaviors
How: Factors that affect motivation, ability, or support of the ASHA
Where: Where are the key touchpoints between ASHAs and beneficiaries located? Where are rituals and focal behaviors of concern situated in the maternal space and how does this affect influence, accessibility, or other factors needed to adopt an effect health-outreach strategy?
Project RISE organized data collection methods around a model meant to capture embeddedness, lived experience, and connections among sources of influence and beliefs. Part of this was approaching this complicated system with a nested model of interactions, which helps document the cultural ecology of health, surrounding perinatal decisions and experiences in Bihar. As shown in Figure (0.2), we have specific objectives at each level. This conceptual tool was used to design the questions in our interviews and quantitative survey.
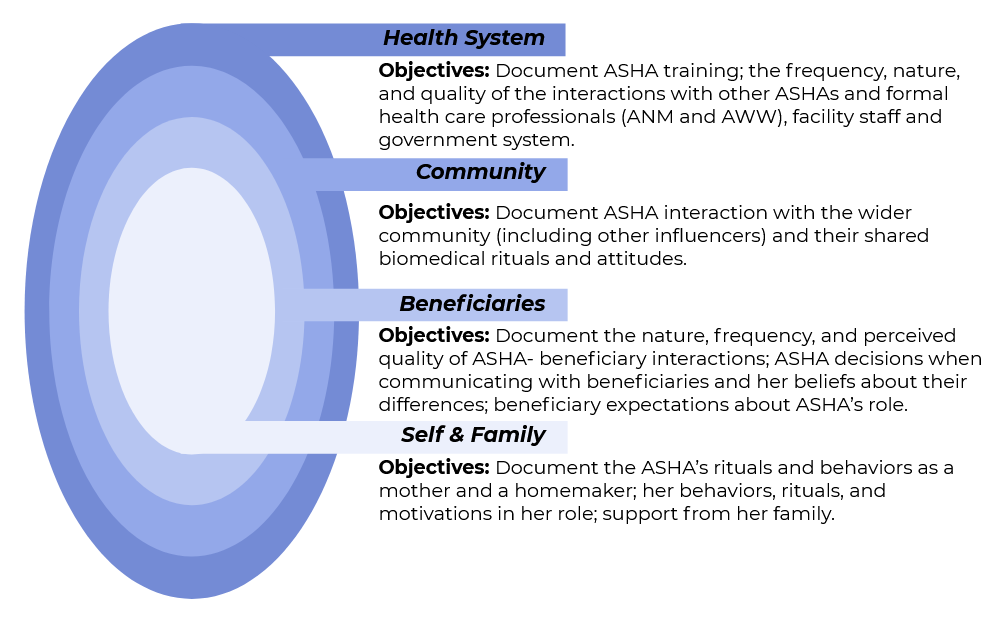
Figure 0.2: Project RISE nested research design and objectives
To adopt a ritual lens and achieve a broad cultural-ecological understand of the complexities of ASHA life, Project RISE used a mixed-methods approach to collect data on many topics: Maternal nutrition; immunization; ASHA training; ASHA interaction; community perceptions of ASHA; ASHA intrinsic and extrinsic motivation; challenges encountered by the ASHA; community and household rituals; ASHA perception of the health care system; sources of influence behind the decisions to practice a wide range of behaviors that surround pregnancy and birth; the associated reasons or causes behind the decisions to practice a wide range of behaviors that surround pregnancy and birth; the process of reasoning about persuasion and messaging in achieving improved health outcomes; demographics like caste, age, and religion of ASHAs and beneficiaries.