0.12 Dai – ASHA Comparison
One of the first indications that ASHAs are often in a liminal state came during synthesis of the qualitative data (Chapter 3), where participants indicated that some behaviors were out of reach to the ASHAs because they were more ‘outside the home,’ whereas Dais2 were ‘inside the home.’ This inside/outside distinction was observed in many ways across datastreams and we realized that it contained insight into how influence can be affected by traditional norms that in turn affect access and even perceptions of relevance. This led to an extensive comparrison of ASHAs and Dais, which in turn reflected some of Project RISE’s key themes regarding the importance of lived-experience, the connectedness of behaviors, and liminality.
Figure 0.7 gives an overview of the qualitative and quantitative findings for these ASHA-Dai comparisons. In both our focus group discussions with mothers (Chapter 3) and in our ethnographically themed qualitative investigations (Chapter 4), women reported that the Dai role has been changing but they are still very much a part of the perinatal experience. Analysis of these responses also indicated that the Dai plays a very different role from the ASHA, and the quantitative data also supported this inside/outside the home distinction in terms of the behaviors influenced.
In comparing just these two influencers, there is still a great deal of complexity in the patterns of influence.
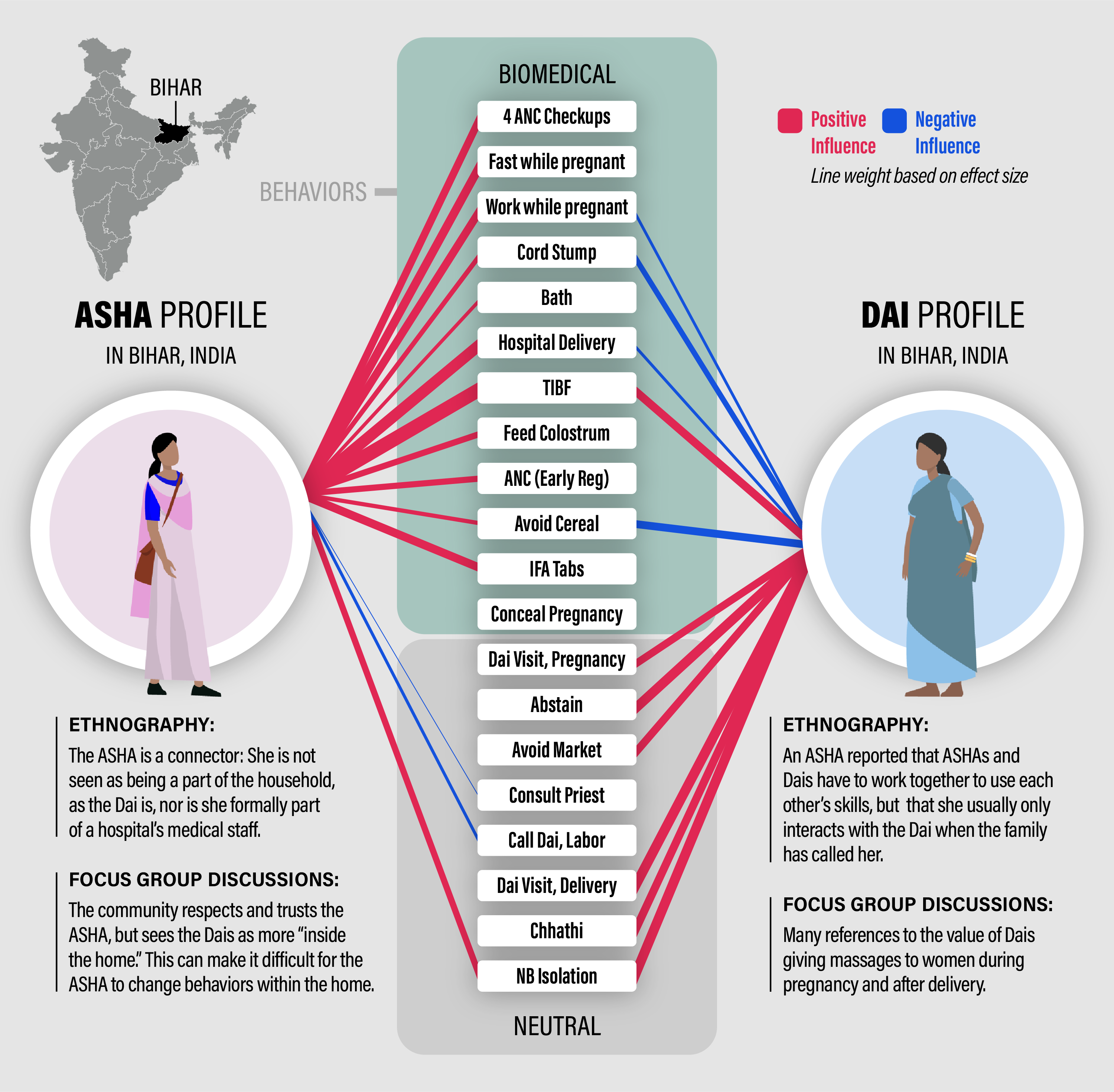
Figure 0.7: ASHA - Dai comparrison: The red lines represent positive effects on the probability that women do the recommended biomedical behavior or do the neutral behavior. Blue lines represent negative effects. These effects are predicted probabilities from a logistic regression. Specifically, the thickness of each line is the difference between the predicted probability for naming an ASHA or Dai as an influencer and naming no one (for description of model and presentation of raw values see Chapter 8). Only effects that have non-overlapping confidence intervals with no one are drawn.
The behaviors in the center of Figure 0.7, show some strong patterns in terms of how they are influenced. First, the behaviors that are connected by a red line to the Dai and the ASHA are positively influenced by both. These include TIBF (timely initiation of breast feeding), and isolating the mother and newborn together postpartum. Of the 19 behaviors pictured, these are the only two that ASHA and Dai both have positive (reinforcing) effects on - meaning that women who name an ASHA or a Dai have highly probabilities of doing those behaviors than women who name no one as an influencer (see Chapter 8 for a full explanation.). There aren’t any behaviors that they both have a negative influence on, but there are a few where they have opposing effects. The Dai increases the probability that women treat their cord stump after delivery, which is not biomedically recommended (Mullany et al. (2009) shows that infections from cord stump treatments can contribute to early life mortality), but women who are influenced by the ASHA tend to not treat their cord stump. The Dai is a strong positive influencer for Chhathi, but a component of Chhathi practiced by some families is to avoid cereal-based food for the first six days postpartum, which is also positively influenced by the Dai. The Dai also increases the odds that women avoid this nutritious food during this critical time (the women certainly eat other nutritious foods) but the ASHA makes them less likely to avoid cereal.
The ASHA has a strong positive influence on every biomedical behavior such that women who name the ASHA as an influence are more likely to align their behaviors in the direction of biomedical recommendations.
Only one behavior is not affected by ASHA nor Dai, concealing the pregnancy. Across our interviews and discussions we found many references to this common desire to conceal the pregnancy from outsiders until the fourth month of pregnancy or longer. Indeed, this is a tendency in much of the world, not just in Bihar. The reasons for this are many but include shyness as well as a fear of evil eye. The ASHAs were just as likely to conceal their own most recent pregnancies as were the mothers in the communities they serve (see Section 8.6 in Chapter 8). This is likely a very resistant behavior.
In this brief example we learned about the different positioning of the ASHA and Dai by analyzing patterns in the behaviors that they are connected to. Our measure of ‘connection’ here is the result of a statistical model that accounts for many possible contributors to variation in behavior (details in Chapter 8). We also see, in terms of the lived experience of the mother, that there are aspects of her perinatal journey where the ASHA doesn’t have much reach, or much of a presence. Limitations in accessibility should also be implemented into messaging and behavior change interventions.
References
Dais are traditional birth attendants, similar to a midwife.↩︎