0.9 Data Types and Methods
Project RISE investigates a series of complex social topics (motivation, health behavior, ritual) with an applied objective to modify behavior and improve health. This requires a strong empirical foundation that includes accurate descriptions of health behaviors, community rituals and beliefs, and the way influencers and cultural values shape health behavior. These endeavors require a mixed-methods approach.
| Qualitative | Quantitative |
|---|---|
| Ethnography: detailed ASHA-focused information based on six weeks of fieldwork | Survey/questionnaire: 1200 recent mothers and 400 ASHAs |
| Focus group discussion: 107 recent mothers and 106 mothers-in-law, for 20 FGDs each | Behavioral vignettes: 291 mothers and 146 ASHAs |
| Key informant interviews: 12 ASHAs, 11 AWWs, 10 Dais, 6 Pandits, 5 Maulanas, 7 RMPs | |
| Interviewing the interviewer: Two remote FGD sessions with five expert informants from Project RISE data collection team |
These datastreams were designed to complement each other as we build a synthetic picture, and their collection occurred in four phases. The first phase included qualitative discussions (FGDs and KIIs) and the ethnography, which provided deep personal perspectives and nuance that in turn informed the content of the second phase: an extensive quantitative survey. Both previous datastreams contributed to the design of behavioral vignettes in the third phase. The behavioral vignettes, short stories that include contextual information about a decision related to a key project outcome, further explored themes identified in the previously collected data. By controlling the content of vignettes, Project RISE could experimentally examine the impact of particular information on how participants reason and make judgments.
Interviewing-the-interviewers:
Additionally, near the end of Project RISE data synthesis, a forth phase of special interviews were conducted to fill out the description of the perinatal ritual landscape and the many complex decisions and inputs Bihari mothers encounter as they progress from just before pregnancy to just after delivery. The ‘interviewers’ who were the subject of these interviews were members of the trained professional data collection team (PCI International, Bihar) who conducted the project’s focus group discussions, key informant interviews, quantitative data collection, and the vignettes. In addition to this Project-based expertise, they have experience conducting many other maternal health projects in Bihar and are Mothers from Bihar themselves. As such, these experts presented a wealth of highly relevant content knowledge. Furthermore, these investigators are themselves mothers in Bihar who have pesonal connections to and knowledge of the local ritual landscapes. The ‘raw data’ from this effort are in Chapter 5, and are the foundation for the synthetic overarching ritual narrative in Chapter 11.
0.9.1 Sample overview
Results by method and datastream are presented in the main text in Chapters 3 through 9. Here we present a brief sample overview and a few illustrative examples chosen to illustrate key project themes. For instance, comparing the behaviors influenced by the ASHA and the Dai, along with community perceptions of their roles, was an early line of evidence highlighting the ‘between’ nature of the ASHA role. We then give an overview of the many lines of evidence regarding ASHA efficacy to show the pathways and behaviors that currently have the highest impact.
Table 0.1 gives an overview of some demographic factors of the women who completed the Project RISE quantitative survey (1200 Mothers and 400 ASHAs). These help acquaint the reader with the data analyzed in later chapters and give a general impression of the populations of interest. The table gives the most common values. Note that the majority of ASHAs and Mothers are Hindu, but that a much higher fraction of Mothers are Muslim (see Chapter 6 for more detail). Similarly for Caste, the most common response for both is OBC but more Mothers (31%) are Scheduled Caste than ASHAs (17%) (and more ASHAs are General Caste).
The other differences give the expected impression that ASHAs are older (by 14 years) and more likely to be literate and have higher levels of education. The most typical parity for the Mothers sample is 1 child, but this is a function of age, as most of the Mothers are young.
| Descriptor | ASHAs | Mothers |
|---|---|---|
| Age | 38 yrs | 24 yrs |
| Age of youngest child | 13 yrs | 2.2 months |
| Religion | Hindu | Hindu |
| Caste | OBC | OBC |
| Education | 10 yrs | 0 yrs |
| Literacy (%) | 100 | 51 |
| Children | 3 | 1 |
| Experience | 10+ yrs | NA |
We also compare the self-reported frequencies of ASHA and Mothers for the behaviors they practiced in their most recent pregnancy (Figure 0.3). Differences between ASHAs and Mothers could be due to a variety of factors, age differences in particular. The largest difference between ASHAs and Mothers is the proportion who had their most recent birth in a hospital (institution), which has increased by over 40% from ASHAs to Mothers. This is likely in part due to the ASHA program itself (the maternal experience of many of the ASHAs did not include an ASHA).
We see other signs of increased compliance with biomedical recommendations from ASHAs to Mothers (with Mothers being more compliant), such as increased ANC Registration, a reduction in bathing within 24 hour, and a reduction in applying substances to the cord stump. One exception in these self-reports is the proportion reporting to have taken the full IFA regimen. Perhaps it is noteworthy that many more of the Mothers who did not complete their IFA dosage reported that they partially completed it. Especially traditional or normative behaviors, like practicing Chhathi or concealing the pregnancy for the first few months, are practiced at nearly identical proportions in each sample, which we interpret as a sign of stability. More descriptive detail on these, and other, health behaviors can be found in Chapter 7 and detailed analysis of how they are influenced in Chapter 8.
This is just a representative sample of the behaviors described in later chapters of this report.
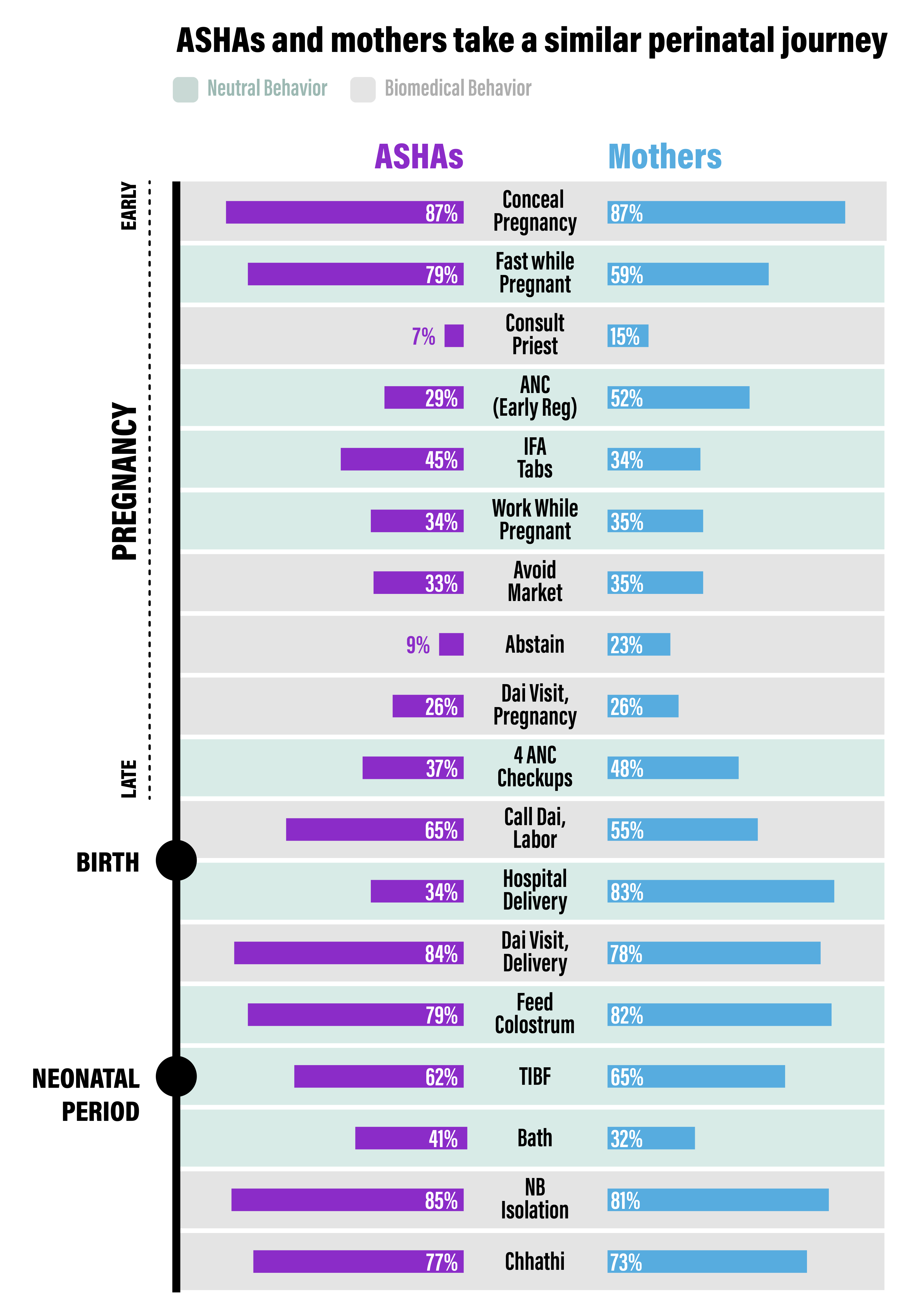
Figure 0.3: Comparison of Mother and ASHA responses about behaviors practiced during their own most recent pregnancy.