10.3 Phase I. Discovery: Understanding the Present
10.3.1 Purpose and Process
The purpose of using HCD in the Discover Phase was to support the framing of the research around ASHAs and the communities that they serve, and to frame the findings from the Mixed Methods Approach around the challenges that ASHAs and their beneficiaries face. The insights from the project were framed as opportunity areas and helped us to build the foundation for the rest of the project.
Discover research and analysis was carried out iteratively from the beginning of the project in March 2019 through to the end of the project in April 2021. The following visual gives an overview of the process, key activities and outputs. The activities and results have been further elaborated on in the subsequent sections.

10.3.2 Defining Research Objectives
Our first step in the project was to define the research objectives. To inform this process, we started with extensive literature review of the project setting in Bihar, including demographic patterns, socio-economic conditions, the health indicators and the health system, specifically the role of ASHAs in that context and the ASHA program success and challenges.
The Scope and UT Austin research teams convened in Helsinki in June, 2018 to discuss the key findings that arose from the literature review. The teams were able to narrow the focus for Project RISE to specific research areas that would have the potential to add to the global body of knowledge regarding ritualization of health behaviors, and such that would have significant implications for the health of women and infants in Bihar.
The Scope and UT Austin teams conducted a field research trip to Muzaffarpur district, Bihar in August, 2018. The aim was to help further ground Project RISE in the context of Bihar state and validate (or invalidate) the learnings emerging from the desk research. Our research objectives, therefore, were quite broad:
- To map the local view of the pregnancy journey: rituals, and traditional and new behaviours that dot the journey.
- To build an initial understanding of the life and work context of the front line workers: their routines, tools at hand and touchpoints with the community.
- To observe and understand the context of health care in Bihar, including the community and the healthcare space.
Based on the agreed research areas we developed a research plan and designed research tools to be used for collecting data in the field. During the trip the two teams worked in parallel and met with a diversity of research participants including women and their families, health care providers, ASHAs, Anganwadi workers (ANW), Auxiliary Nurses and Midwives (ANM), and other key influencers. The research methods included in depth interviews, group discussions, key informant interviews, and observations. All interactions with research participants were audio recorded and transcribed (from the local language to English) by the in-field partner- Project Concern International (PCI).
After the field trip, we reviewed the transcripts, and organized all the gathered data in order to find patterns and themes. This helped to identify compelling insights and consistent gaps that emerge from the data, based on which we were able to gradually carve out our research objectives.
To help organize our thinking of the ASHA and her world and the collected data we utilized the ‘Nested-Social-Ecology Model’ described earlier in this report (2.6.1). As mentioned, the nested approach breaks down the complex environment that ASHAs occupy into levels that describe significant influencers for the ASHA and her work: 1) self and family 2) beneficiaries 3) community and 4) health care system. We then used these levels to organize research objectives so as to enable understanding of the interaction within and between them, as illustrated below.
10.3.3 Mixed method research and data collection
Project RISE collected data using both quantitative and qualitative methods including ethnography, focus group discussions, key informant interviews, in-depth large-scale surveys, and behavioural vignettes to study ASHAs in context. These methods were selected and designed sequentially in a manner that sought to complement the strengths of each method. The RISE team met at regular intervals to make sense of the incoming data from a human-centered perspective to identify relevant themes to focus further as the research progressed.
10.3.4 Mixed Method Analysis
The analysis process was a highly iterative and collaborative process that took place throughout the project, in parallel with other project stages informing and feeding into the different activities. To analyze our research findings we applied a mixed method analysis approach, which is a procedure for analysing data that includes coding, sorting and clustering to find patterns, connections and relationships, and identifying themes. HCD was used to run Pre-design sessions in July and August, 2019 to synthesise the emerging findings from mixed methods analysis on to a ASHA-centered framework. As we kept synthesising more and more data, we continued iterating the framework to finally arrive at a version that highlighted how ASHAs embedded role in between the community and the health system results in tensions and opportunities in her personal and professional life.
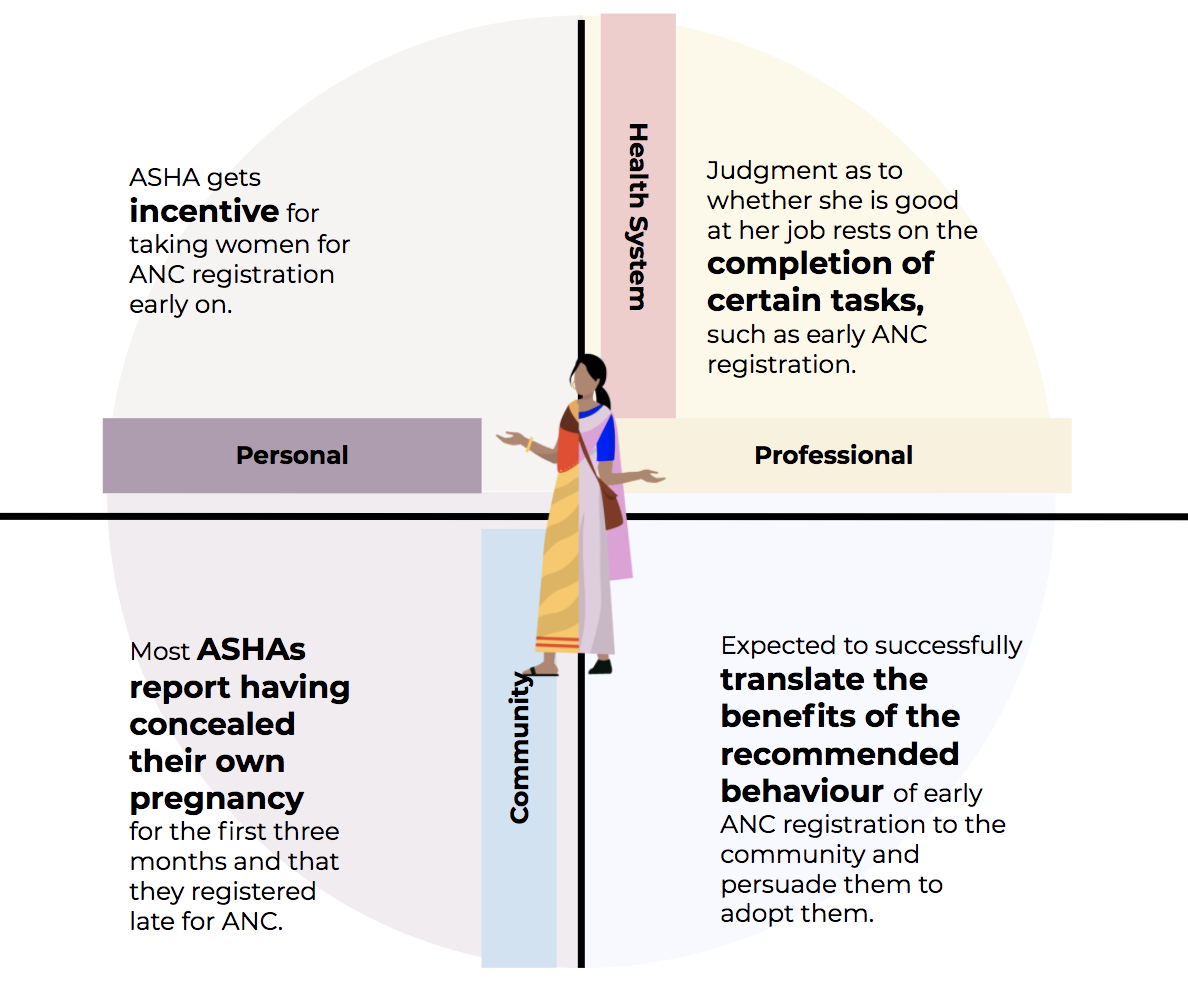
10.3.5 Data Synthesis through Four Domains
An ASHA operates between the Health System and Community, with one foot in each of them. ASHA, who is also a woman from the same community thus has two different but overlapping roles - personal and professional - that cut across the community and the health system.
Due to her unique placement as a CHW, the expectations and requirements of these four domains are intertwined and feed into each other. However, the competing expectations and requirements in each domain give rise to a series of tensions that usually go unrecognized and unresolved by the health system. To structure our understanding of ASHA dynamics we mapped out how the expectations and requirements of her role interact across four domains.
10.3.6 Four Opportunity Areas
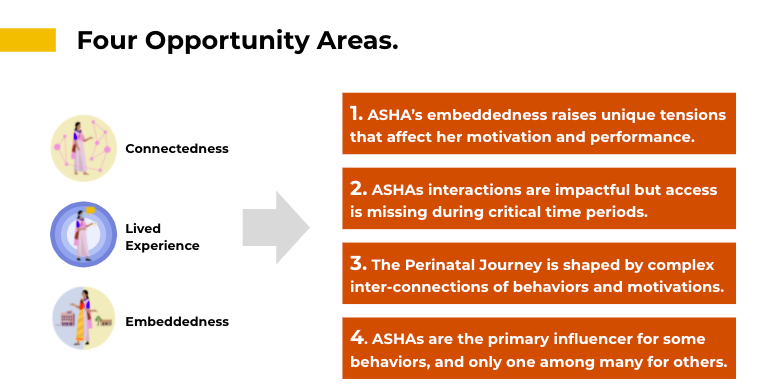
The synthesis of the research findings and the identified patterns of tensions ASHAs experience across the four domains helped us identify four Opportunity Areas for leveraging rituals and devise solutions to improve the ASHAs motivation and performance. These are outlined in the table below.
The opportunity areas detail key hidden truths brought out by patterns of beliefs, attitudes, and behavior, or articulate the Aha moments, based on data found during research. They also reflect limitations i.e. unmet user needs, unresolved problems or other tensions identified through the analysis and synthesis process. The opportunity areas are directly linked with the Role of ASHAs and the implications that stem from adopting a ritual lens and embracing the complexity that surrounds behavioral norms. These are namely the 1) Connectedness of behaviours 2) Lived Experience of ASHAs and the 3) betweennees of the of ASHA’s role that derive from their embeddedness in the community they serve as CHWs and tensions that it may bring about.
The purpose of these Opportunity Areas is to leverage the understanding that has emerged from applying the rituals lens to the ASHA Role and the health behaviours of the communities that they serve, and to inspire new solutions that resolve the tensions in her embedded role and enable her to be a better ‘culture facilitator.’ The details of these opportunity areas and the data streams that they are derived from can be found on these slides (Link to Opportunity area slides).
ASHAs role viewed through a ritual lens
- Connectedness
Behaviors do not exist in isolation. They may be connected to many other behaviors, beliefs, and sources of influence that interact in complex ways. In order to develop an effective strategy, these connections need to be documented and understood. Doing so can identify opportunity areas or barriers for behavior change.
- Lived Experience
An ASHA’s personal experience as a mother and member of the community shape her approach to the job and her motivation. Differences between ASHAs and beneficiaries shape opportunities, barriers, and messaging for interventions. ASHAs are mothers and like all of us they draw from their own experiences and perceptions. Understanding this provides a vantage point into her approach, perceptions, and opens up different opportunities for intervention.
- Being in Between
CHWs are from the communities where they work. The ASHA bridges worlds between the outside and inside. This creates underappreciated tensions as she must change behaviors of people she lives near by bringing in external viewpoints. This embeddedness affects ASHA motivation and behavior in complex ways that should not be ignored.
Opportunity areas and opportunities for action
- ASHA’s embeddedness raises unique tensions that affect her motivation and performance.
Support ASHAs resolving tensions in her professional and personal life:
Resolve tensions and in her personal and professional life that arise due to her embeddedness between the health system and community.
Clearly define ASHA’s positioning and strengthen her status within the health facility staff and the community members, to allow her to build trust, respect, and self-efficacy.
Enable ASHAs to extend their role from that of Service Extender to Culture Translator:
- Provide ASHAs tools and training to leverage her lived experience and employ her understanding of the community norms and practices to be an effective persuader regarding behaviour change practices.
(The next three opportunity areas build further on this)
- ASHAs interactions are impactful but access is missing during critical time periods.
Engage mothers with ASHAs early and often:
Engage mothers at the earliest possible time with ASHAs.
Increase the frequency of ASHA interactions.
Engage when the perceived risk of evil eye and impurity is low and ASHA has access to the mother.
Enable ASHAs to be an effective persuader and behaviour change agent:
Enable ASHA to tackle perceived risks and leverage relevant motivations of the community like avoiding miscarriage.
Enable ASHAs to leverage and augment relevant rituals and traditional practices with biomedically recommended health advice for better health outcomes.
- The Perinatal Journey is shaped by complex inter-connections of behaviors and motivations.
Enable ASHAs to put their knowledge of community into practice by leveraging the interconnected links between behaviours and motivations, to become an effective persuader and behaviour change agent.
Enable ASHAs to identify the right timing to reach out to mothers and families to influence behaviours, when their access is not occluded by other behaviours or norms.
For the same motivation of preventing risk and promoting health of the child, there can be contradictory biomedical and traditional practices. Enable ASHAs to understand the connections between behaviours functions and motivations.
Enable ASHAs to identify key motivations of mothers and their families that decide whether a behaviour is practiced or not.
Enable ASHAs to leverage normative and biomedical behaviours that families are already practicing, and tap into their motivation, to shape the uptake of other biomedical behaviours.
- ASHAs are the primary influencer for some behaviors, and only one among many for others.
When biomedical behaviours are in conflict with normative behaviours, we require holistic, interwoven strategies:
For biomedical behaviours, like ANC registration, ASHA has strong positive influence, and doesn’t directly compete with other influencers.
In normative behaviours like bathing the child within 24 hours, ASHA’s advice competes with many local influencers including, family, friends and relatives and Dai.
A biomedical behaviour (early ANC registration) might be in conflict with a strong normative behaviour (concealing pregnancy). Therefore, ASHA might compete indirectly against other influencers in biomedical behaviours.
When normative behaviours are in conflict with biomedical recommendations, it is very important for ASHA to:
- align with and leverage other local health influencers.
- Leverage earlier biomedical or traditional behaviours when there is no conflict.
- Tap into the most relevant motivations of the mother and the family.