2.6 Organizing Concepts
Based on the above rationale and description of Project RISE goals, it is clear that the scope and complexity is rather vast. In order to design project methods in ways that key concepts could be articulated across data streams, a few structuring concepts were needed.
At the beginning of the project, we used a ‘nested-social ecology’ to orient our thinking about the ASHA and her world, which we describe in the next section. After extensive synthesis and discussion this was further distilled to the domain-quadrants diagram, which we use as a visual conceptual tool to highlight tensions and synergies in the social dynamics that shape the ASHA world.
2.6.1 A Nested-Social Ecology
ASHAs occupy a complex space influenced by many social, economic, and political factors. To break this complex ecology down into manageable parts we developed a nested approach for studying the levels of ASHA interaction (Fig. 2.1).
The four nested levels, or spheres, are described as follows:
Self & Family: The ASHA’s personal experiences, rituals, and behaviors as a mother and a homemaker. This includes her personal background and how her household and family dynamics relate to her role as an ASHA.
Beneficiaries: The women in the ASHA’s catchment area who receive her services. This sphere includes the nature, frequency, and perceived quality of ASHA - beneficiary interactions as well as how ASHAs communicate with beneficiaries and beneficiary expectations about the ASHA’s role.
Community: The broader community to which the ASHA and beneficiaries both belong. This includes interaction with other influencers and their biomedical rituals and attitudes.
The health-care system: The ASHA, the community, and the beneficiaries are, to a degree, nested within the health-care system (some aspects of their decision making and behaviors can be considered as ‘nested’ in this way, but certainly not all of them). At this level we focus on ASHA training, the frequency, nature, and quality of her interactions with other ASHAs, and formal health care professionals (ANM and AWW).
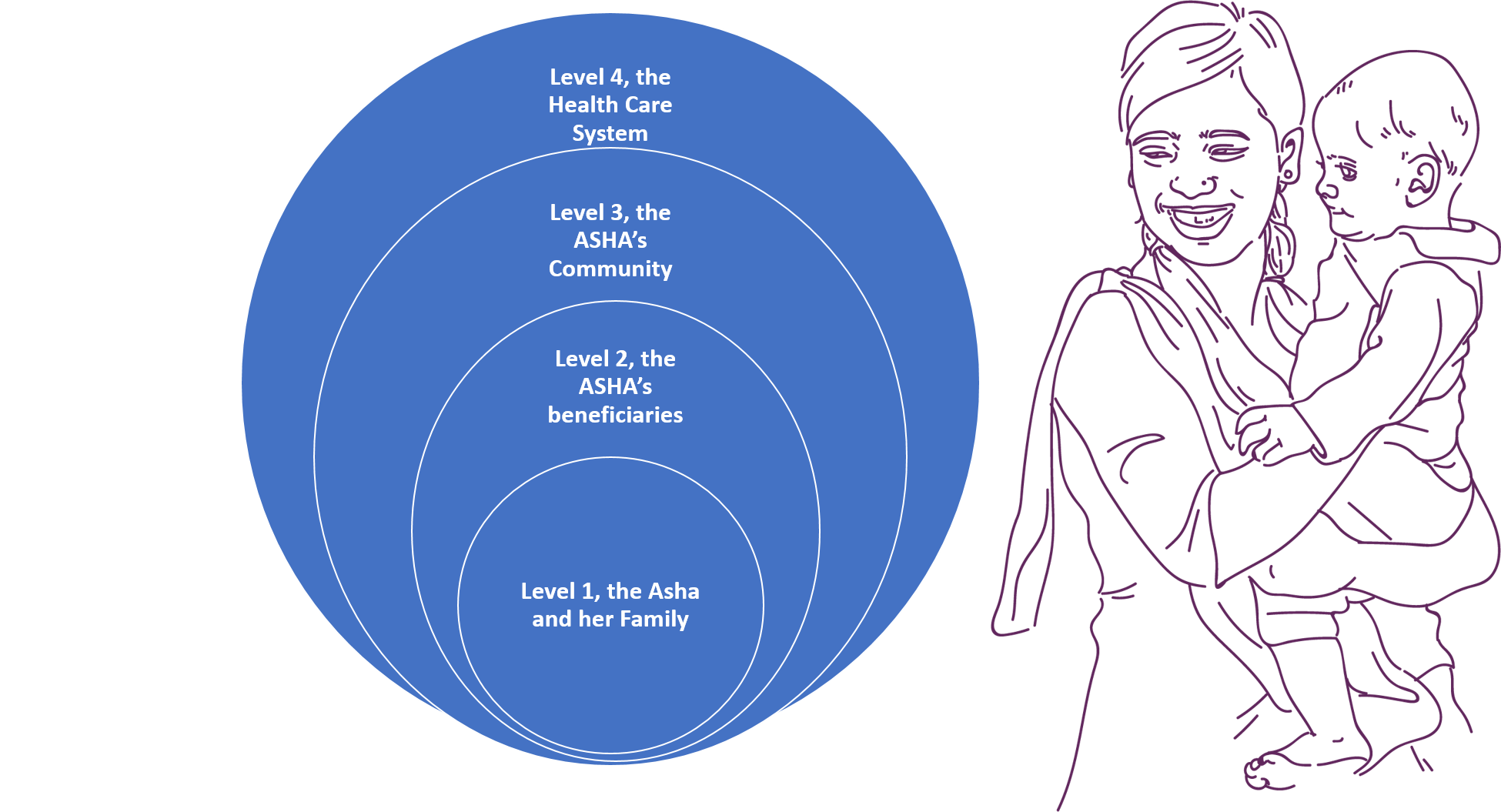
Figure 2.1: Nested-Social-Ecology: Conceptual figure of ASHA’s four main spheres of interaction.
This diagramatic framing was highly useful for organizing our thinking, especially early in the Project when we were designing the mixed-methods approach. It helped ensure that we included key interactions at all of these levels in our questionnaire and in the vignettes, and allowed us to examine how the levels interact or how tensions in the expectations or behaviors among them might create barriers to ASHA performance.
2.6.1.1 Influencers and Reasons
Part of understanding the role of rituals, beliefs, knowledge, and practices in shaping both ASHA motivation and her interactions with beneficiaries requires documenting the constellation of influencers and sources of information around health behavior. To compliment the nested ecology design illustrated in Figure 2.1, Project RISE asks, where possible, about sources of influence and the reasoning behind decisions about whether or not to engage in a certain behavior. For example, the quantitative survey has several questions similar in form to: when you were pregnant with your last child, did you take IFA tablets? but covering a wide range of scenarios and behaviors. Each of these is associated with a ‘who told you to do that?’ and a ‘why did you do that?’ Patterning across these responses will reveal which individuals or information sources are most immediately associated which behaviors. We can address connections between behaviors and reasoning, which can in turn inform about messaging or existing cultural associations between cause and effect for various perinatal behaviors.
2.6.2 Insights hiding in plain sight
While synthesizing and discussing Project RISE data, it became increasingly clear that some fundamentally important, and previously under-scrutinized, parts of the ASHA’s role are fairly mundane aspects of her role description. Because these things were ‘there all along’ but had under-appreciated implications for how we understand her motivation and performance, we consider them insights hiding in plain sight.
The first of these is her role as a connector between the community and the health care system. This places the ASHA in an unusual situation because the boundaries between home life and work life are blurred and overlapping. In many ways, this is part of the strength of her position, and it is part of the rationale for why CHW programs exist in the first place.
This means that the ASHA is often in a liminal7 state, connecting but not fully part of two worlds.
This means that the ASHA is often in a situation where she is connecting, but not fully part of, two worlds.
In particular, she helps families but is not inside the household. She brings beneficiaries to the health system, but when she is in the hospital she is treated as an outsider and is not a doctor. This dynamic is critical to understanding ASHA behavior and motivation. Again, the Indian Government’s Rural Health Mission of 2005 states– ASHA would act as a bridge between the ANM and the village and be accountable to the Panchayat – and as such, the notion of the ASHA as a connector is in the very definition of her role. Yet, the implications for how this affects the nature of her work, her motivation, and her relationship with the community is not widely appreciated in evaluations of the ASHA program nor by attempts to design interventions to improve her performance from a social-and-behavior-change perspective.
Second, the ASHA has two different but overlapping roles - personal and professional - that cut across the community and the health system. For example, people who work in offices can have fairly non-overlapping social interactions between their office life and their non-work or home life. The very nature of the ASHA role is that her personal life is embedded within the community where she works. Her personal domain and her professional domain interact in ways that will affect her performance and her motivation. This subtle point may be critical to understanding ASHA dynamics.
The realization of the importance of these two concepts led to the construction of the diagram in Figure 2.2.
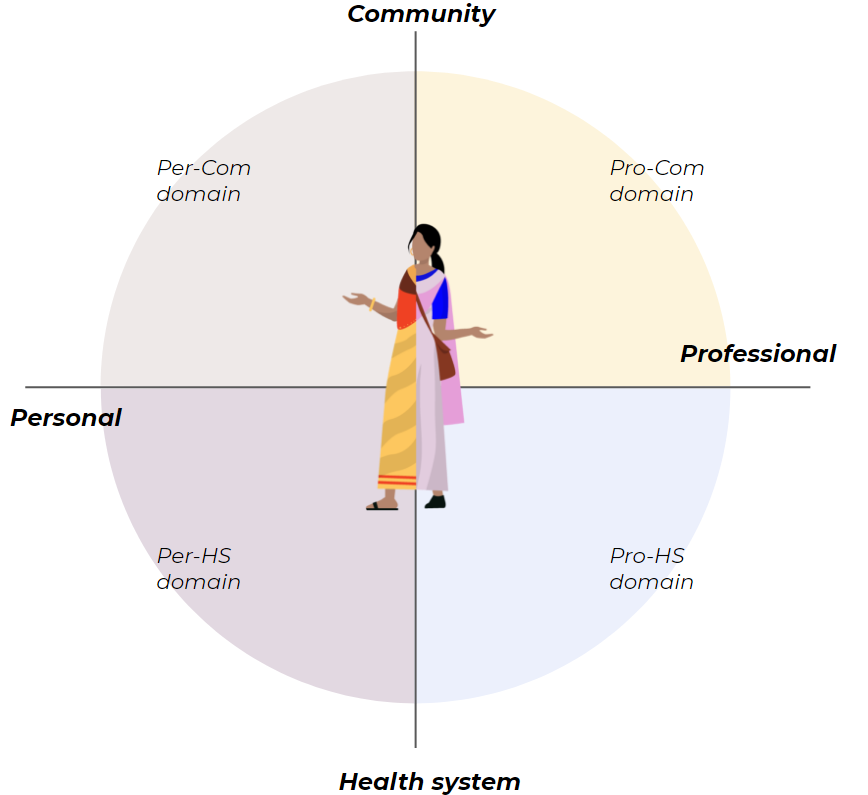
Figure 2.2: Domain quadrants: Conceptual figure of the main axes of variation that reveal tensions among norms, expectation, and behaviors in the ASHA’s world as a community member and a service provider
Take-Home Messages: Organizing Concepts
- To structure our understanding of ASHA dynamics we map out her interactions on the quadrants shown in Figure 2.2.
- One axis highlights the dual domains of personal life, the lived experience and household requirements of the ASHA as a community member, mother, and woman in Bihar, in contrast with the professional role of ASHA as a service provider. The fact that ASHA’s live in the communities she provides services to is a top-down motivation for CHW programs but this apparent aspect of ASHAs has not been fully integrated into interventions or SBCC approaches.
- The other axis contrasts the nature of the ASHA’s role as a connector. She connects beneficiaries to the health care community but is not a member of the households she serves nor is she a member of the health care community. This can create all kinds of hidden barriers and obstacles to her performance and motivation that need to be understood in much greater detail.
formally, liminal means being in an intermediate state, phase, or condition (Webster’s dictionary). In Anthropology the concept is similar, but includes the sensation of disorientation or ambiguity that accompanies this status as being intermediate, or in between, states, identities, or communities. Further, anthropologists have noted that the state of being liminal may describe a time just before a ritual transition marking membership of the new state or rite of passage from one identity to another.↩︎