12.4 Mixed Methods Case Study: From concealing the pregnancy to IFA tablets
As an example of connections among behaviors and influencers, we take an in-depth look at consuming IFA tablets, ANC registration, and concealing the pregnancy.
IFA tablets are an important dietary supplement that is critical in an area where maternal nutrition is often a concern and where various factors may limit access of pregnant women to adequate supplies of food (fasting, customs about women eating after men have finished their meals, a belief that eating too much makes the baby too large, etc). Reasons to not take the recommended dosage of IFA include that they can cause digestive problems that lead to discomfort, but also supply issues can limit their adequate distribution. Moreover, the messaging emphasizes the role of iron but may under-emphasize the importance of folic acid. IFA tablets were mentioned in the key informant interviews with Dai, RMP, and ASHA, but did not come up in any of the 40 FGDs with mothers and MILs. The majority of these references (across Dai, ASHA, and RMP), were promoting the consumption of taking IFA tablets or were simply stating that they are something that is or should commonly be done. One Dai said they were only for weak women.
In our sample of Mothers, only 34% took the full recommended IFA regimen, 52% registered for ANC in a timely fashion, and 87% concealed their pregnancy (Table 7.2). In comparing the lived experience of ASHAs to Mothers, and in examining the work-life dynamics within ASHAs (Table 7.5), we found that concealing the pregnancy is an especially ‘rigid’ behavior, meaning that most women are likely to do it. In addition, there were no frequently named influencers who raised the probabilities that women revealed their pregnancies early, among ASHAs nor Mothers (Figure 8.9).
Likewise, there are many reasons tied to the desire to conceal the pregnancy. These include shyness and a fear of evil eye (Chapter 3). This common tendency of concealing the pregnancy was referred to during KIIs with ASHAs, AWWs, and a Dai, and in FGDs with mothers and MILs. ASHAs said they did recommend hiding the pregnancy from outsiders (but not from ASHAs) for up to five months. Evil eye and shyness were stated as reasons not to reveal the pregnancy to outsiders. AWWs also mentioned evil eye as a reason to hide the pregnancy and one AWW thought that pregnancy is hidden within Hindu communities. Dais also recommended hiding the pregnancy for risk of evil eye, as did a few mothers and MILs.
The desire to conceal the pregnancy in turn may share some connections to broader proscriptions against movement during pregnancy. There are many instances in the qualitative data saying that pregnant women should not roam around or go to markets or be outside for fear of the jiloi bird or perhaps that via witchcraft a jealous women could steal a mother’s pregnancy by pulling a thread from her sari (Chapter 11). As such, there is a great deal of deeply rooted hesitation around revealing the pregnancy or having pregnant women go out into the open and these hesitations derive from coexisting beliefs. From a biomedical perspective, concealing the pregnancy in and of itself is an understandable and non-problematic behavior, but doing so can create problematic delays in other key services. Moreover, around the time of when a woman might find out she’s become pregnant tends be when ASHA access to the woman is limited. So the ASHA may need ways to message that occur before the pregnancy or there need to be mechanisms by which a young and newly pregnant woman can contact an ASHA without otherwise divulging to others that she is pregnant. General delays in revealing the pregnancy to outsiders lead to specific delays in notifying the ASHA of the pregnancy, which in turn delays the ANC registration which in turn lowers the probability that IFA tablets are taken at the recommended dosage (it also delays the start of taking IFA, which is important to take early in pregnancy). Among Mothers, very few register for ANC early (about 12%) and the majority register in the third month (~44%), but over 1/4 register in the fifth month onward (not counting the few who don’t register at all).
| Month range | Proportion |
|---|---|
| 0-2 | 0.12 |
| 3 | 0.44 |
| 4 | 0.18 |
| 5-9 | 0.26 |
The ASHA has no effect on the probability that mothers reveal their pregnancy early (and perhaps shouldn’t be expected to), but has a strong positive influence on ANC registration and taking IFA. Moreover, mothers who register for ANC late are much less likely to mention the ASHA as a source of influence (Figure 12.6).
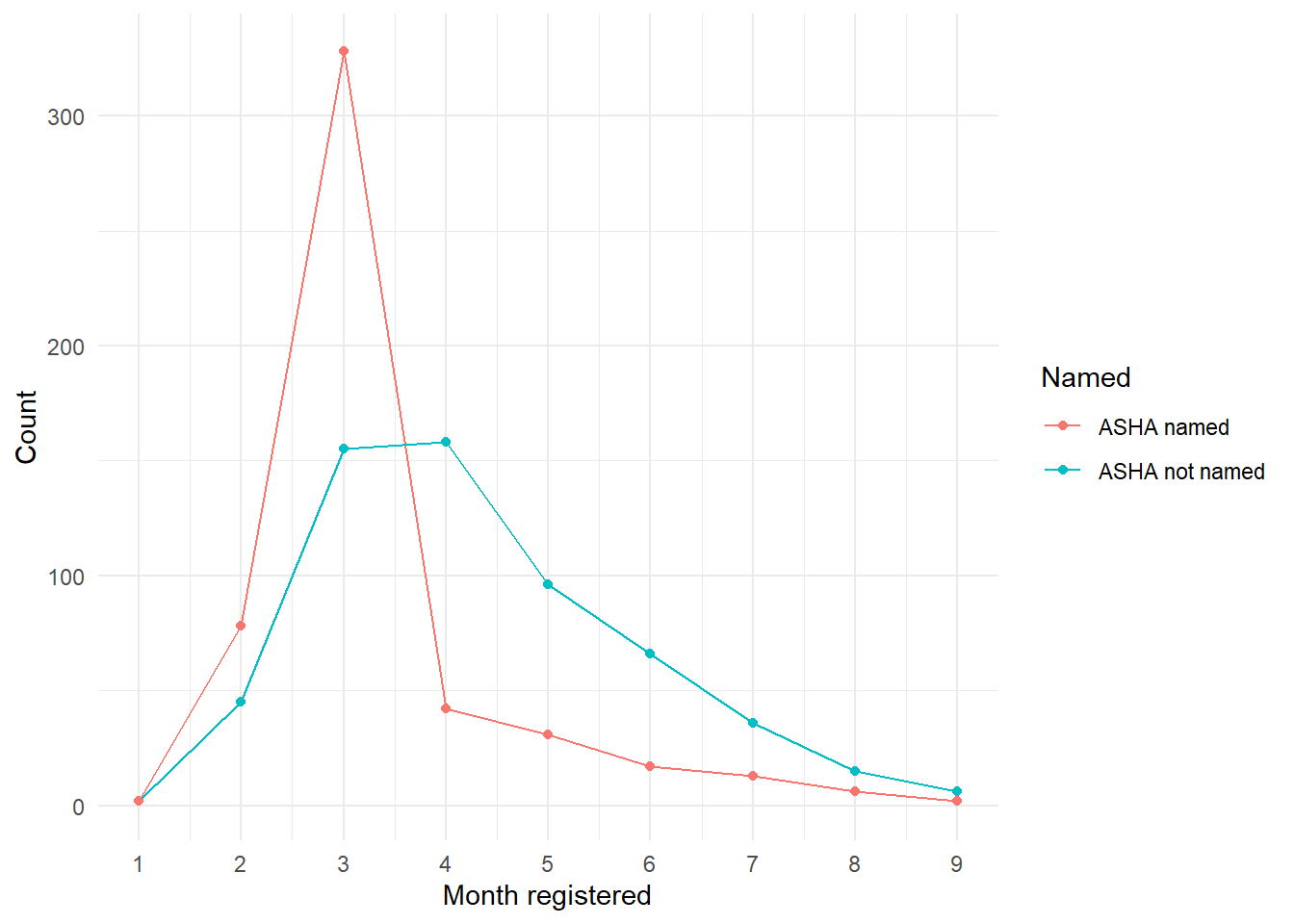
Figure 12.6: Mothers who named an ASHA compared to those who did not, by month of ANC registration.
In Table 12.2 we see the top seven most common given reasons for not giving the recommended response to each behavior. For not registering for ANC the top response is “I believe in the importance of the registration,” which may seem confusing but keep in mind that many of these women are registering in the 4th month, may not have been aware of exactly which month they got pregnant, and see this as a timely registration. The other responses cover issues with service providers, normative compliance, and incomplete information.
The top reasons for concealing the pregnancy are that these Mothers didn’t feel it was necessary or felt shy to do so, followed by several normative responses (every does so, neighbors do so, etc.). The next two most-common responses are a fear of evil eye and a lack of awareness for the pregnancy.
Reasons for not taking IFA tablets include a lack of supply, not feeling they were necessary (at times specifically because the woman felt healthy), normative responses, a lack of information, and a fear of the side effects.
| Reason | n |
|---|---|
| ancreg | |
| I believe in the importance of the registration | 294 |
| Came to know about pregnancy after 3 months | 152 |
| Doctor/nurse/asha delayed/refused | 149 |
| I did the same in the previous delivery | 136 |
| Other | 127 |
| Everybody does in the family | 113 |
| I didn’t know about registration | 99 |
| hidep | |
| Donìt feel necessary | 438 |
| Feel shy to disclose the pregnancy | 263 |
| I did the same in the previous delivery | 234 |
| Everybody does in the family | 205 |
| Neighbors/relatives also do | 164 |
| To save the child from evil eye | 137 |
| Came to know about pregnancy after 3 months | 132 |
| ifa | |
| I donìt believe in the importance of consuming ifa | 483 |
| Side effects(burning sensation, giddness, loose motions | 301 |
| Did the same in the previous delivery | 295 |
| Ifa tablets/syrup were not available | 219 |
| Nobody does in the family | 162 |
| Did not need as i was healthy | 154 |
| Did not know about ifa tablets | 126 |
In contrast, Table (12.3) gives the reasons stated by women who did the recommended behavior in each case (meaning they did early ANC registration, took full IFA tablets, or revealed their pregnancy in the first three months). We see lots of awareness for the benefits of each action, some normative responses, and a desire to receive the services.
| Reason | n |
|---|---|
| ancreg | |
| I believe in the importance of the registration | 598 |
| To avail anc services | 425 |
| Everybody does in the family | 391 |
| I did the same in the previous delivery | 344 |
| Neighbors/relatives also do | 313 |
| To ensure health of the child in the womb | 198 |
| To avail govt. Schemes | 153 |
| hidep | |
| I believe the importance of early revelation | 153 |
| I did the same in the previous delivery | 108 |
| Everybody does in the family | 104 |
| Neighbors/relatives also do | 71 |
| To avail anc services | 24 |
| Others | 19 |
| Reduces pregnancy related complications | 19 |
| ifa | |
| I believe in the importance of consuming ifa | 399 |
| To increase blood level in the body | 297 |
| To ensure health of the child in the womb | 260 |
| Did the same in the previous delivery | 201 |
| Everybody does in the family | 186 |
| Reduces risk of pregnancy related illnesses/complications | 181 |
| Neighbors/relatives also do | 149 |
In order to remove the barrier of a concealed pregnancy, the ASHA either needs a way for Mothers to contact her discretely, which also would probably require an established and trusting relationship beforehand. As we saw in the ritual narrative (Chapter 11), there is not a lot of contact with the outside world early in the pregnancy, and the months leading up to that pregnancy may also be somewhat secluded if the woman is in a new household and village. Thus, ways to establish a relationship with a woman’s new ASHA could be explored.
The women taking IFA seem to associate it fairly commonly with the health of their developing child. Increasing awareness of this could be a useful messaging strategy, as women who do not take often feel that they needn’t do so if they feel healthy.
These three behaviors are connected and any intervention concerned with only one of them would likely not be successful as one aware of the connections to and dynamics surrounding the other two.