12.6 Tensions from Liminality
The India Government’s National Rural Health Mission (NRHM) describes the ASHA role as “the interface between the community and the public health system.” Both the focus group discussions and ethnography documented several instances that speak to ASHA as a connector, or as one positioned between systems. Throughout this report we have documented qualitative and quantitative evidence that establishes liminality as a key factor affecting ASHA dynamics. We suggest that being a connector of systems, where one is the community where one lives and the other is a formal government system, needs more exploration from the perspective of improving performance and motivation.
Figure 12.7 shows a conceptual scheme informed by Project RISE data for some ways to ease tensions that emerge from the liminality experienced by ASHAs. Tensions can occur in each of the main quadrants formed by being between health system and community and between her lived-experience and her professional role. We see resolving these tensions as an essential part of facilitating a transition from service extender to cultural facilitator.
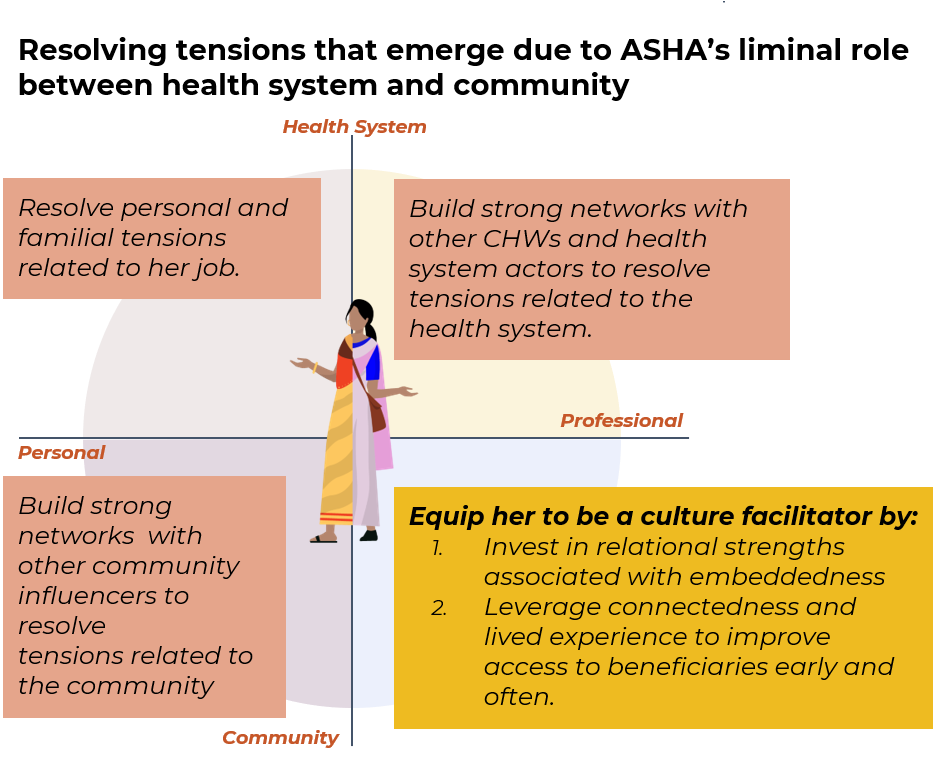
Figure 12.7: Develop a general approach for resolving tensions from liminality that might emerge in each quadrant.
The ASHA program has not fully appreciated the many ways that tensions can result from interactions between the expectations and requirements of her personal and professional roles across the health system and community.
In practice, the health system has limited its focus to the service extender aspect of her role, thus missing out on supporting and building the role of ASHA in engaging in culturally-sensitive health communication or strengthening her relationships and contacts with other stakeholders and CHWs in the community. For example , ASHA trainings are based on providing biomedical information but not on how to navigate the social dynamic in the household, adapting messaging based on the motivations of the family and community and leveraging other health influencers in the community.
Some specific tensions:
- Health facility staff tend to perceive ASHA as an intermediary, and not necessarily as an extension of health system in the community. ASHAs are perceived as someone who does not have a role in service delivery beyond bringing the community to a service touchpoint. This establishes an unequal power dynamic that manifests in the facility staff exhibiting behaviors such as demanding bribes, and treating her disrespectfully. ASHAs reported experiencing disrespectful behavior when making requests from the health providers with regards to their payment. This kind of treatment at the facility leads to a loss of face for the ASHA in the community, where it is imperative that people take her seriously, for her to accomplish the tasks that are set out for her.