Chapter 10 Respiratory System
We need respiration to move air in and out of our lungs to facilitate gas exchange between the lungs and the capillaries and the capillaries and the tissues.
Gas transport occurs between the tissues and the lungs.
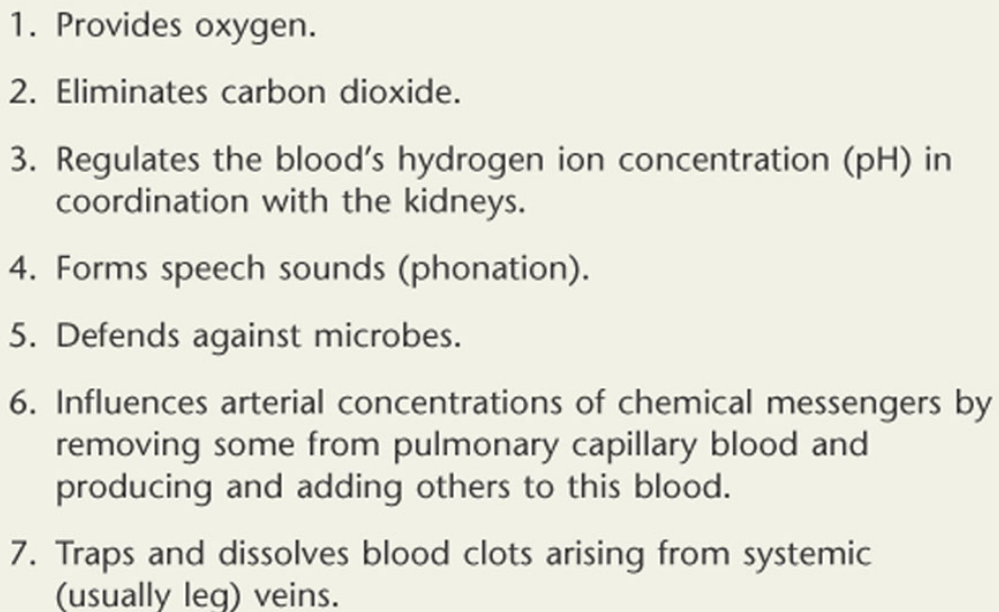
Figure 10.1: Functions of the Respiratory System
The pulmonary alveoli is the functional unit of the lungs.
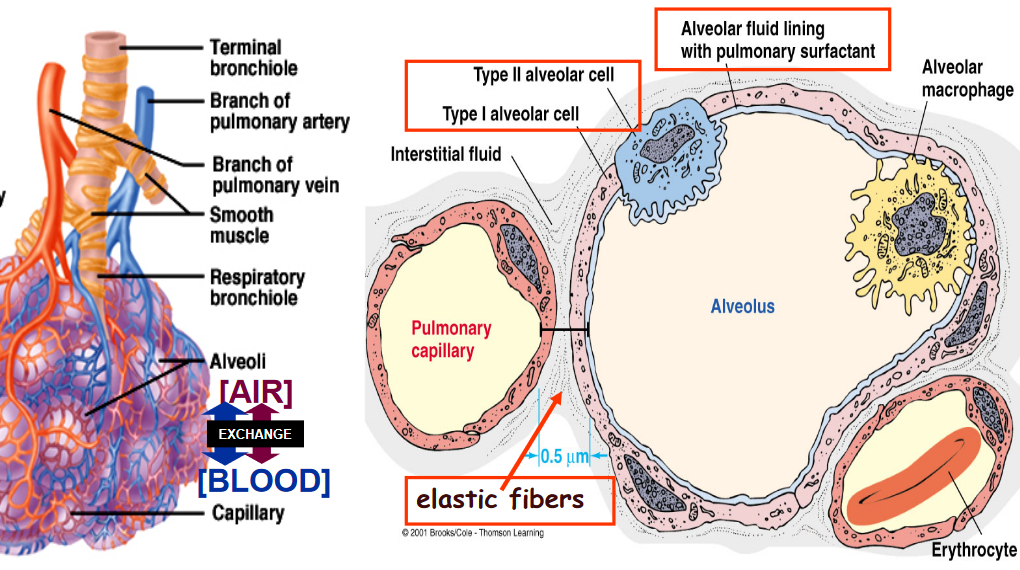
Figure 10.2: Functional Unit of the Lungs
10.1 Properties of the Lung
Compliance in the lung is due to the vast amount of elastin protein fibers present.
Compliance is a measure of lung expansion. Lungs are a 100 times more distensible than balloons.
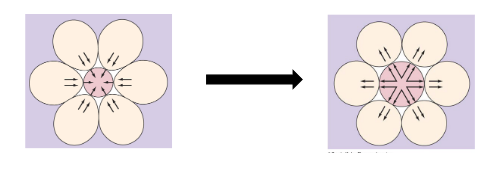
Figure 10.3: Alveolar Distension
Elastance is the tendency for lungs to recoil after distension. When an alveolus collapses, its neighboring alveoli recoil to pull and expand the collapsing alveoli.
10.1.1 Pulmonary surfactants
Surfactants help reduce surface tension on the alveoli.
Surface tension is a force generated by water’s attracting force - this force resists distension (i.e., the alveolus stays collapsed).
Pulmonary surfactants, on the contrary, are complex phospholipid proteins that are secreted by type II alveolar cells. These reduce surface tension and increase compliance.
Also note Laplace’s law - given the surface tension \(T\) and the alveolar radius \(R\), the inward pressure of an alveolus is:
\[\begin{equation*} P = \frac{2T}{R} \end{equation*}\]
Hence, pulmonary surfactants decrease surface tension on the alveolus and prevents it from collapsing.
10.1.2 Respiratory distress syndrome
This happens when a newborn lacks adequate amounts of pulmonary surfactants; this is more common in premature babies and is the cause of death in infants. Consequently, the alveoli in their lungs have much more surface tension and have low compliance.
This can be treated with glucocorticoids and synthetic or natural surfactants through a breathing tube.
10.1.3 Surfactant secretion
Cortisol promotes the secretion of pulmonary surfactants - this was a feat discovered by Graham Liggins in sheep.
He found that the lungs of premature lambs sunk in water - they are only inflated if cortisol was injected into to ewes (i.e., female sheeps).
Antenatal glucocorticoid therapy is now used to treat high-risk infants and newborn respiratory-distress syndrome.
10.2 Pulmonary Pressures
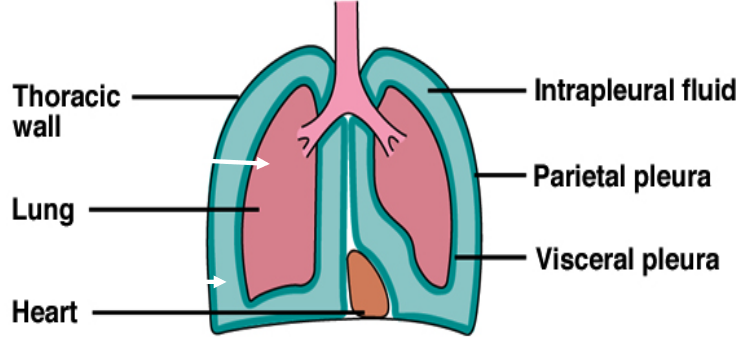
Figure 10.4: Pulmonary Pressures
The atmospheric pressure is around 760 - the pressure in the 756 at rest and changes with respiration.
The intrapleural fluid’s cohesiveness and trans-pulmonary pressure gradient holds the lungs and the thoracic wall in tight apposition so that the lungs fill the thorax.
Pneumothorax occurs when the transmural pressure gradient is lost:
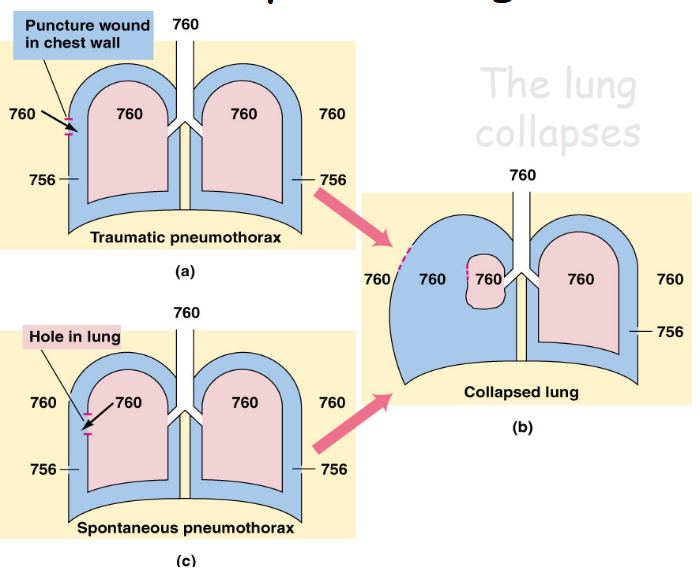
Figure 10.5: Pneumothorax Mechanism
Ventilation is a result of change in pulmonary pressure. Boyle’s law states that pressure \(P\) is inversely proportional to volume \(V\); in other words:
\[\begin{equation*} P \sim \frac{1}{v} \end{equation*}\]
Hence, a greater lung volume results in lower pulmonary pressure - by the law of diffusion, air diffuses down its pressure gradient into the lungs and vice versa.
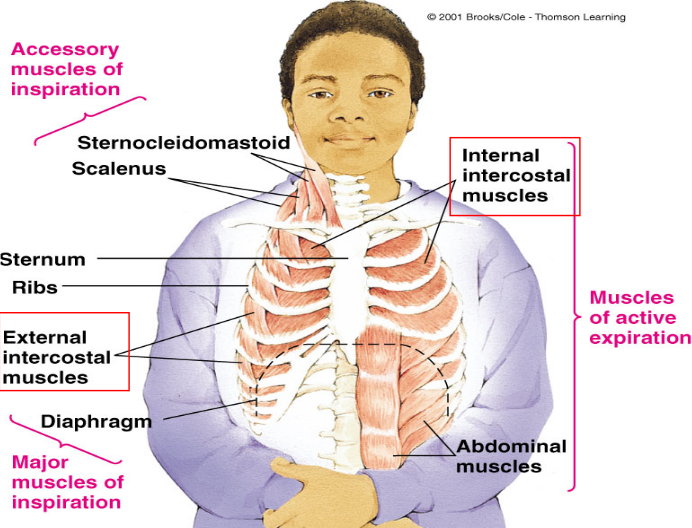
Figure 10.6: Muscles of Respiration
10.2.1 Inspiration
During inspiration, there is the contraction of the diaphragm and the external intercostals to expand the rib cage.
During forceful inspiration, accessory muscles raise the sternum and the first two ribs to expand the upper thorax.
10.2.2 Expiration
The external intercostals relax and so does the diaphragm. The lungs also recoil.
During active expiration, internal intercostal muscles contract to reduce front-to-back dimensions of the thoracic cavity. The abdominal muscles then contract to push the diaphragm upward
10.3 Pulmonary and Alveoli Ventilation
Anatomical dead space refers to the volume of air in conducting pathways.
The pulmonary ventilation rate is given by the product of the tidal volume and the respiration rate:
\[\begin{equation*} \text{Pulmonary Ventilation = tidal volume} \times \text{respiratory rate} \end{equation*}\]
Alveoli ventilation rates can be calculated via the following formula:
\[\begin{equation*} \text{(tidal volume - dead space volume)} \times \text{respiratory rate} \end{equation*}\]
10.3.1 Controlling airway resistance
The hormone epinephrine and sympathetic stimulation causes bronchodilation and reduced secretion via the \(\beta 2\) adrenergic receptors.
Furthermore, parasympathetic stimulation causes bronchoconstriction and increases secretions via the muscacrinic receptors.
An increased amount of CO2 causes bronchodilation; histamines and cold air causes bronchoconstriction.
10.3.2 Types of pulmonary disorders
10.3.2.1 Obstructive pulmonary disorders
These are caused by an obstruction along the airway passage - asthma, chronic bronchitis, and emphysema are all examples of obstructive pulmonary disorders.
Alveolar damage can result from these types of disorders!
10.3.2.2 Restrictive pulmonary disorders
These disorders are characterized by reduced compliance. Pulmonary fibrosis (i.e., the accumulation of fibrous lung tissue) and asbestosis (i.e., an inflammatory and fibrotic lung disease caused by inhaling abestos dust) are such examples.
10.4 Gas Exchange
All gas exchange in the human body follows Fick’s law of diffusion:
\[\begin{equation*} R = AD \times \frac{P_1 - P_2}{d} \end{equation*}\]
Where:
- \(R\) is the rate of diffusion across a membrane
- \(A\) is the surface area
- \(D\) is the diffusion coefficient of a particular gas
- \(d\) is the distance
- \(P_1 - P_2\) is the partial pressure difference
10.4.1 What is partial pressure?
Each gas exerts a pressure that is proportional to its concentration in the mixture - the individual pressure of each gas is called the “partial pressure.”
Note that gases always move down their concentration gradients.
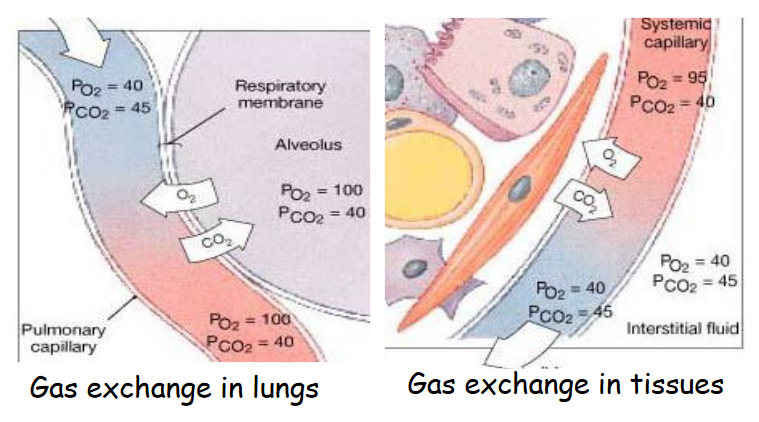
Figure 10.7: Gas Exchange in the Human Body
10.5 Gas Transport
Hemoglobin (i.e., “Hb”) is responsible for O2 transport - Hb increases the O2 carrying capacity by 65 folds!
10.5.1 O2 Disassociation Curve
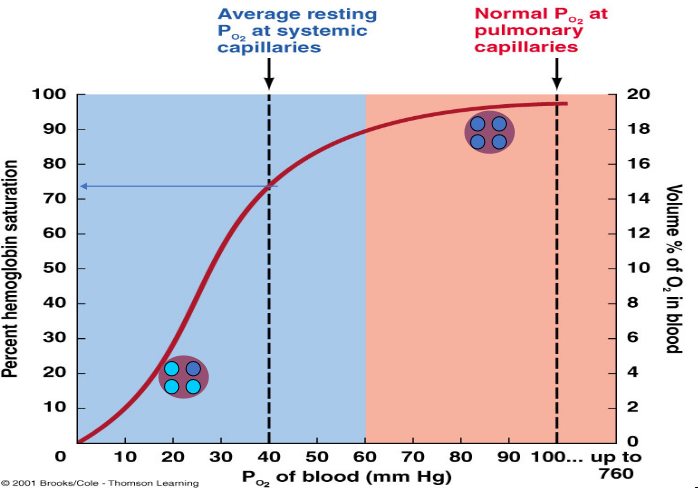
Figure 10.8: O2 Disassociation Curve
The partial presure of oxygen in the blood determines the percentage of Hb saturation. The upper plateau of the curve ensures that if the partial pressure of oxygen exceeds 60 mm Hg, that it doesn’t alter the blood’s supply of oxygen significantly.
This is in contrast to the lower portions of the curve: this portion facilitates the release of oxygen in the capillaries surrounding the tissues. The Hb saturation is 75% at the partial pressure 40 mm Hg. Hence, a further fall in the partial pressure causes O2 to be readily released from Hb.
10.5.2 Factors affecting the affinity of Hb for O2
Bohr’s effect states that CO2 and acid in the blood decrease the binding affinity of Hb for O2, hence facilitating the release of O2.
Hb’s affinity for CO is at least 240 times stronger than O2 - hence the reason why CO is so dangerous!
Also note that fetal hemoglobin has a higher affinity than adult hemoglobin:
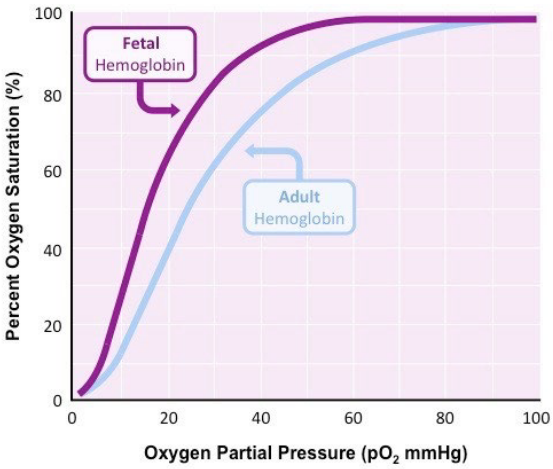
Figure 10.9: Fetal Hemoglobin has a Higher Affinity for O2
10.5.3 CO2 Transport
CO2 is about 10% dissolved in the human bloodstream - 30% of CO2 is bound to the globin portion of hemoglobin, and deoxygenated Hb has a higher affinity for CO2 than HbO2 (i.e., hemoglobin saturated with O2 - this is called Heldane’s effect).
60% of CO2 in the bloodstream exists as bicarbonate ions (i.e., HCO3-):
\[\begin{equation*} CO_2 + H_2O \leftrightarrow H_2CO_3^- \leftrightarrow H^+ + HCO_3^- \end{equation*}\]
10.5.4 Abnormal blood O2 and CO2 levels
Hypoxia refers to an insufficient amount of O2 at the cellular level. Hypoxic hypoxia is due to an insufficient amount of oxygen at the lungs.
Hyperoxia refers to above-normal arterial partial pressure levels of O2 (i.e., PO2).
Hypocapnia refers to below-normal arterial CO2 partial pressure levels due to hyperventilation. This may result in respiratory alkalosis.
Hypercania refers to excess CO2 due to hypoventilation. Respiratory acidosis may result.
There is also apnea and dyspnea.
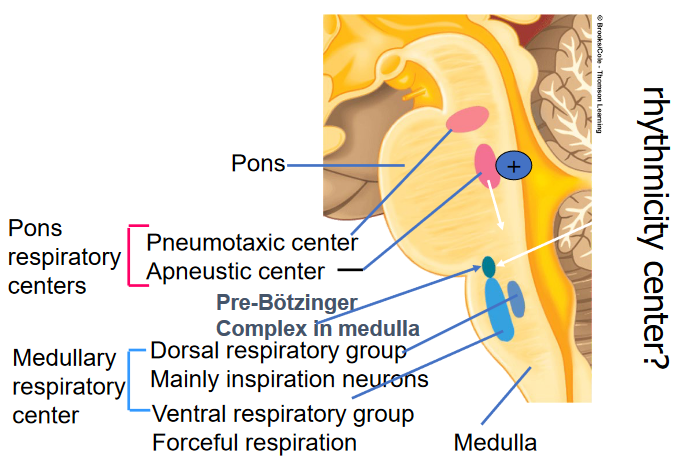
Figure 10.10: Respiratory Centers in the Brain
10.5.5 Stimulants of Respiration
Inspiration (i.e., inhalation) happens when inspiratory neurons fire and activate the motor neurons supplying the inspiratory muscles. Expiration (i.e., exhaling) occurs when these inspiratory neurons stop firing.
During active expiration, the expiratory neurons stimulate the motor neurons supplying the expiratory muscles.
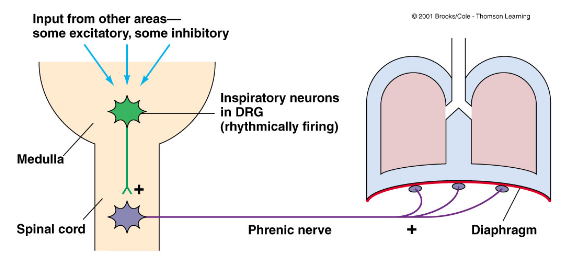
Figure 10.11: Inhaling and Exhaling Activity
Also, be aware of the following:
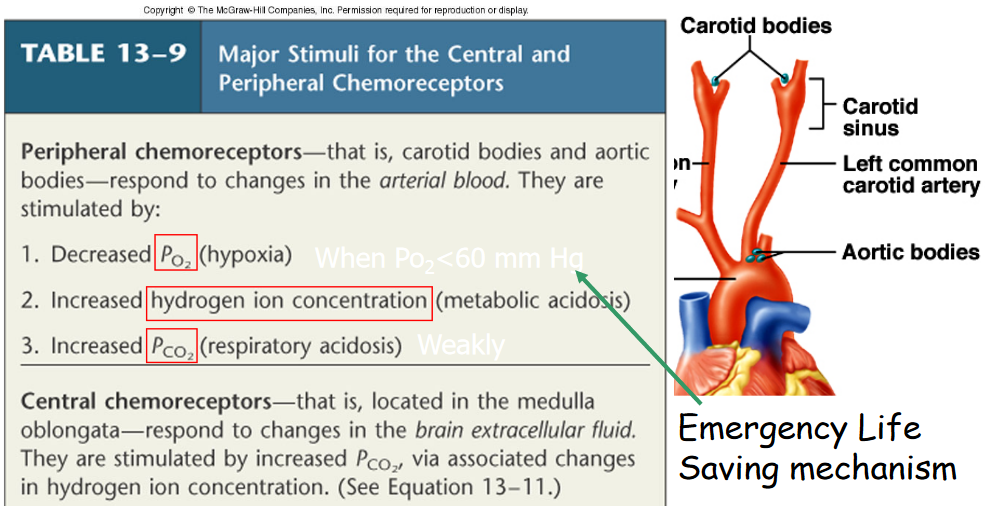
Figure 10.12: Inputs from Chemoreceptors
10.5.6 Adjusting to high altitudes
There is the hypoxic hyperventilation response (i.e., hypocapnia-induced alkalosis). Hypoxic hypoxia also happens as the affinity of Hb for O2 is decreased due to an increase in 2,3-DPG concentrations.
Some other changes include:
- Increased heart rate, stroke volume, and blood pressure
- Increased hemoglobin and red blood cell production due to increased erythroprotein secretion from the kidneys
- Increased lung surface areas
- Increased amount of capillaries