Chapter 12 Renal Physiology II
12.1 Secretion
During secretion, substances are transferred from the peritubular capillaries into the lumen of tubules and into the urine.
Secretion also serves to regulate the concentrations of K+ and H+ in the bloodstream; secretions from the kidney include organic anions and cations.
Maintaining blood K+ levels are crucial for the function of excitable tissues:
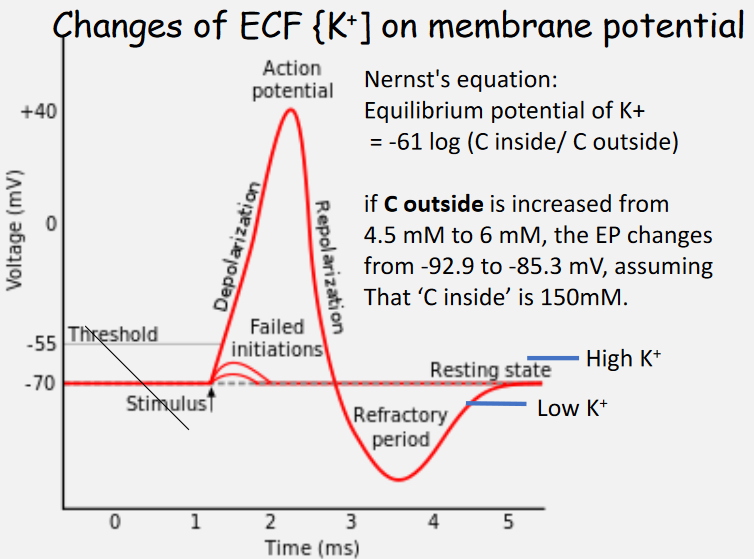
Figure 12.1: Effects of Changing Potassium Levels on Membrane Potentials
12.1.1 K+ secretions
Most filtered K+ ions are reabsorbed at the proximal tubules - as mentioned previously, secretion is needed to maintain blood plasma concentrations of K+.
K+ secretion also happens in the distal and the collecting tubules via the Na+ / K+ pump and is stimulated by aldosterone.
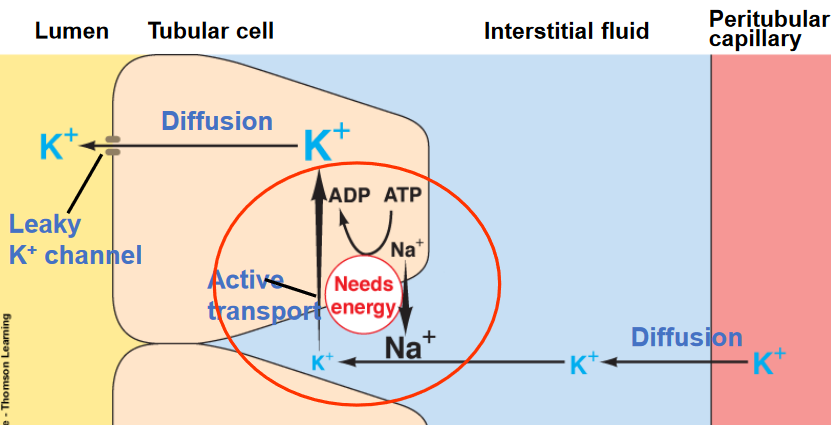
Figure 12.2: Potassium Secretions
The circled region in red represents the Na+ / K+ ATPase in the basolateral membrane of the distal and the collecting tubules. Na+ is transferred into the interstitial space (i.e., reabsorbed) while K+ is transferred into tubular cells before being secreted via leaky K+ channels.
12.2 H+ Secretions and Acid Balance in the Body
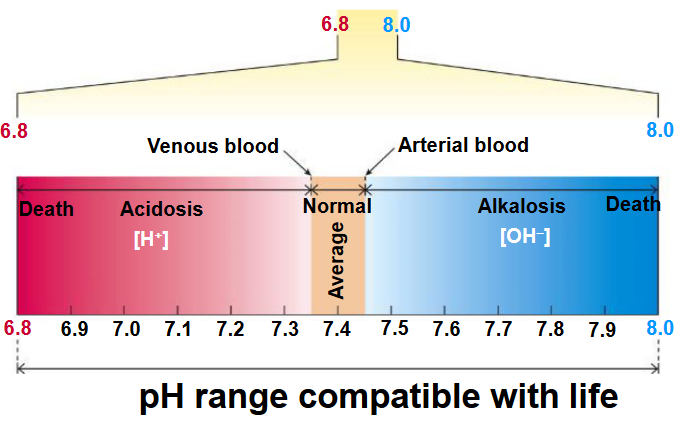
Figure 12.3: Range of pH Suitable for Life
Life has a limited pH range (see above graphic)
12.2.1 Sources of H+
H+ is continuously added to blood plasma from metabolic activities - a major source of H+ is from the disassociation of carbonic acid from CO2:
\[\begin{equation} CO_2 + H_2O \leftrightarrow H_2CO_3 \leftrightarrow HCO_3^- + H^+ \end{equation}\]
Other sources also include (in)organic acids from metabolism!
12.2.2 Defenses against changes in H+ concentrations in the extracellular fluid
While all filtered H+ ions are excreted from the body, most excreted H+ ions are actively secreted. The latter processes happen in the proximal, the distal, and the collecting tubule and are mediated by Na+ / H+ antiporter, H+ ATPase, and H+-K+ ATPase.
However, more important is the fact that H+ secretion can be coupled to HCO3+ reabsorption!
12.2.2.1 Conserving HCO3-
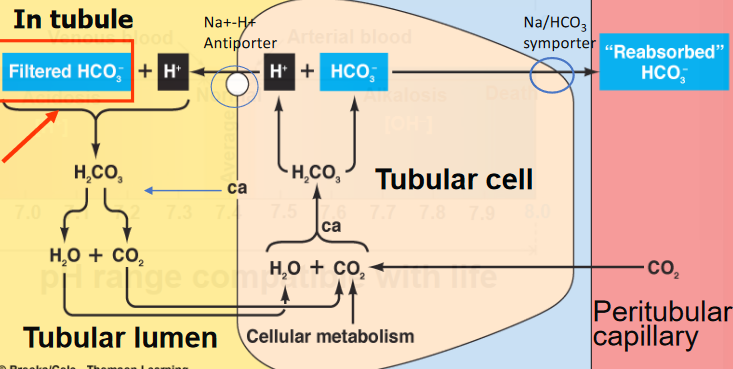
Figure 12.4: Bicarbonate Ion Reabsorption
Most HCO3- ions are reabsorbed at the proximal tubules - filtered HCO3- also reacts with secreted H+ to be reabsorbed.
Note that H+ secretions can also be coupled with the addition of a new HCO3- ion to plasma (see above graphic).
12.2.2.2 HPO42- and NH3
The kidney’s nephrons are unable to produce urine with a pH of less than 4.5 (i.e., the normal pH range for urine is 4.6 to 8 [inclusive]).
Hence, filtered phosphate buffer and secreted ammonia provide a buffering mechanism for the tubular fluid:
\[\begin{align} Na_2HPO_4 + H^+ &\rightarrow NaH_2HPO_4 + Na^+ \\ NH_3 + H^+ &\rightarrow {NH_4}^+ \text{ (lost in urine)} \end{align}\]
Nevertheless, NH3 (i.e., ammonia) is an important buffer in urine: the amount of phosphate secreted is not subject to control! NH3 is made from glutamine in tubular cells in response to excess H+.
12.3 Fluid Balance
The kidneys are capable of producing urine with varying solute concentrations (i.e., 100 - 1200 mOsm / l).
Though, 124 of 125 ml / min of filtrate is reabsorbed - this results in 1.5 liters of urine produced by the kidneys each day.
Note that a small reduction in filtrate reabsorption can have a large influence on urine volume: a 1% reduction in reabsorption can double the volume of urine produced!
12.3.1 Distribution of body fluid
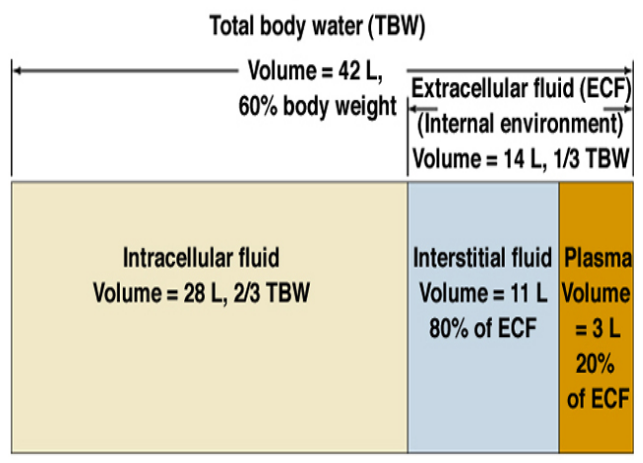
Figure 12.5: Distribution of Body Fluids
12.3.2 Ionic composition of bodily fluids
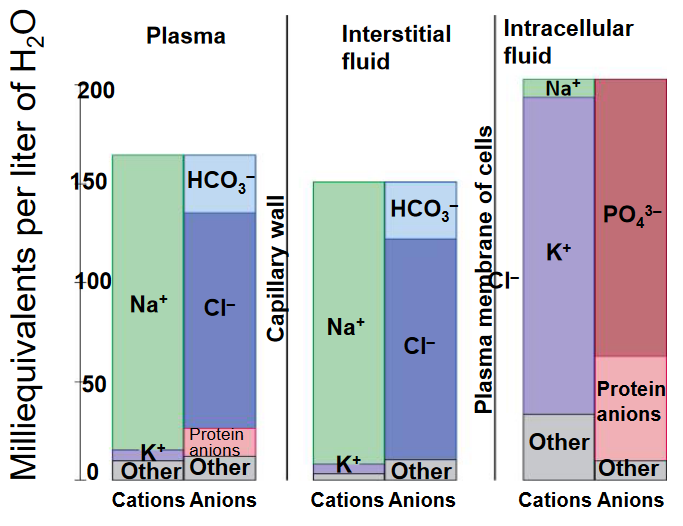
Figure 12.6: Ion Composition of Bodily Fluids
12.3.3 Imbalances in the volume and osmolarity of extracellular fluid
An imbalance in the osmolarity of the extracellular fluid has a tendency to influence the volume of intracellular fluid too.
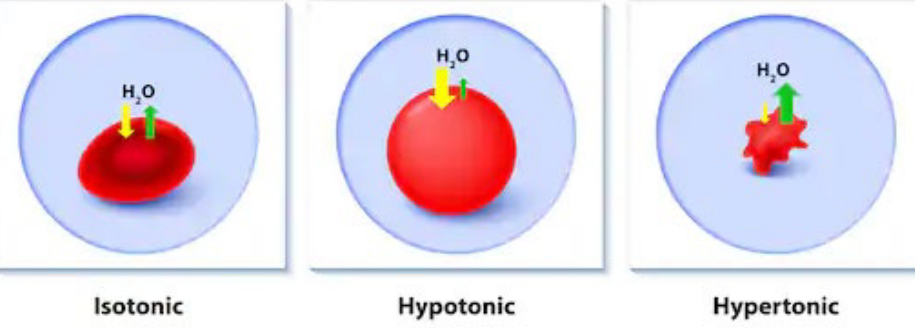
While extracellular fluid volume is important for maintaining proper blood pressure, a hypotonic extracellular fluid causes cells to swell, hence disrupting brain functions.
Hypertonic extracellular fluid, on the contrary, causes cells to shrink. This causes neural dysfunctions, muscle weakness, hypertension, and edema.
12.3.4 Hypertonic and hypotonic solutions
12.3.4.1 Hypertonic solutions
Some causes include:
- Insufficient H2O intake (i.e., dehydration)
- Excessive H2O loss from vomiting, profuse sweating, or diarrhea
- Diabetes insepidus. This is a disease characterized by a deficiency of vasopressin.
12.3.4.2 Hypertonic solutions
- Rapid intake of H2O - hence, the kidneys are unable to eliminate the H2O rapidly enough.
- Too much vasopressing secreted by the body - this could be caused by a disease.
- Renal (i.e., kidney failure)
12.4 Urinary Excretions
The vertical osmotic gradient in the medulla’s fluid enables urine to be secreted at a rate of 100 - 1200 mOsm / L.
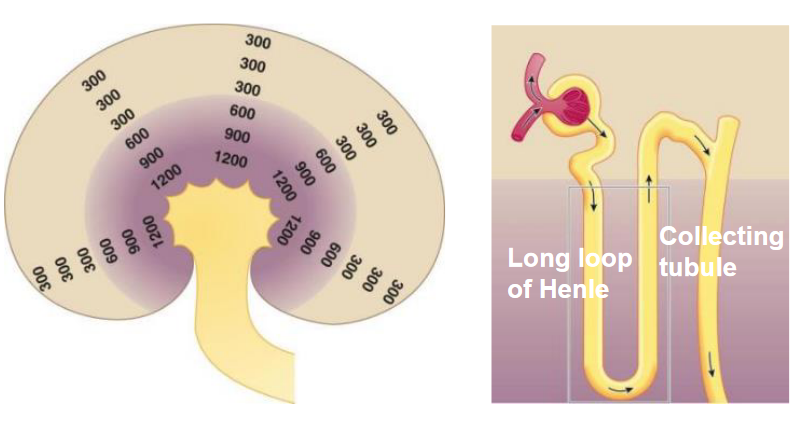
Figure 12.7: The Vertical Osmotic Gradient
12.4.1 Generating the vertical osmotic gradient
A long loop of Henle digs deep into the medulla (near the renal pelvis) - the descending limb of the loop is permeable to water; the ascending limb of the loop is permeable to salt.
The vasa recta (i.e., peritubular capillaries) also dig deep in hairpin loops next to the loop of Henle.
The flow of minerals in both the loop of Henle and the vasa recta run in opposite directions. This is called the countercurrent multiplier system. This system comes from the fact that the flow of minerals in both vessels run in opposite directions; the solute pumps that increase (i.e., multiply) the concentrations of urea and Na+ deep in the medulla.
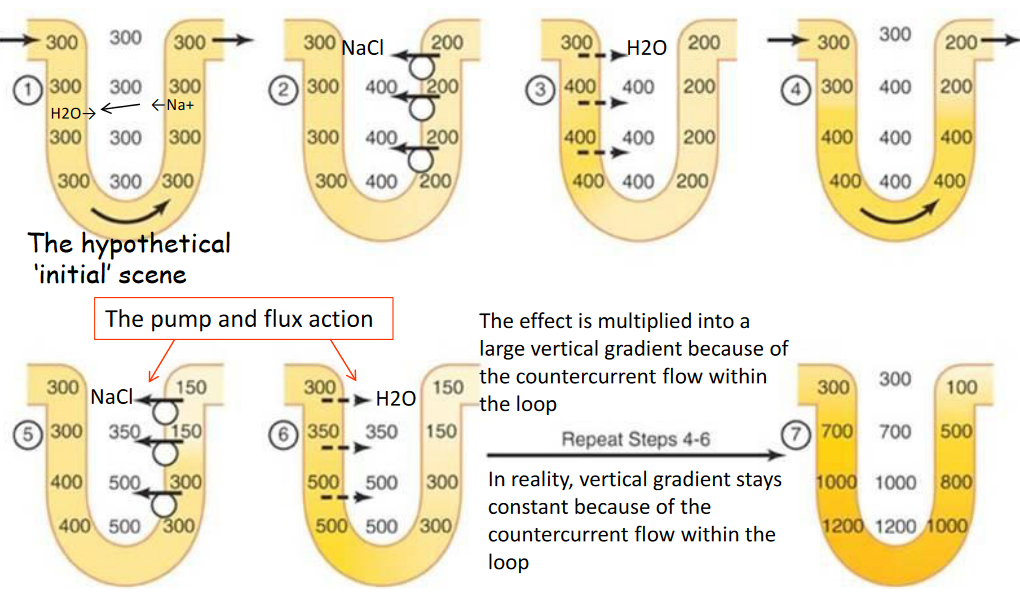
Figure 12.8: Countercurrent Multiplication Generates the Vertical Osmotic Gradient
Similarly, the vasa recta also uses countercurrent exchange to preserve the vertical osmotic gradient:
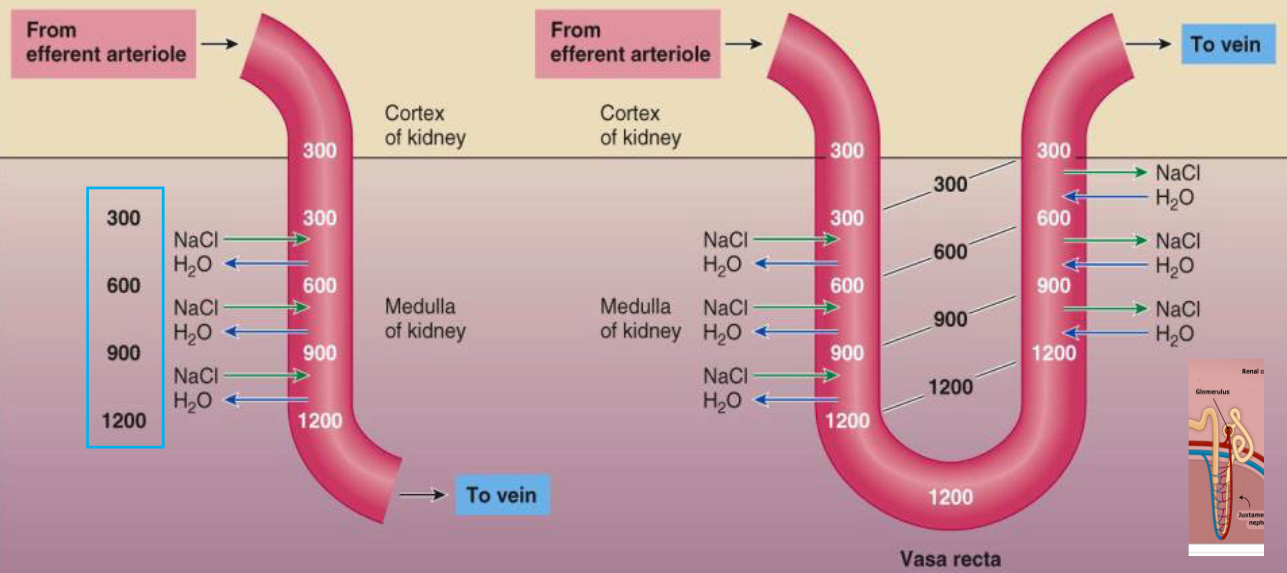
Figure 12.9: Countercurrent Exchange in the Vasa Recta
12.4.2 ADH deficiencies
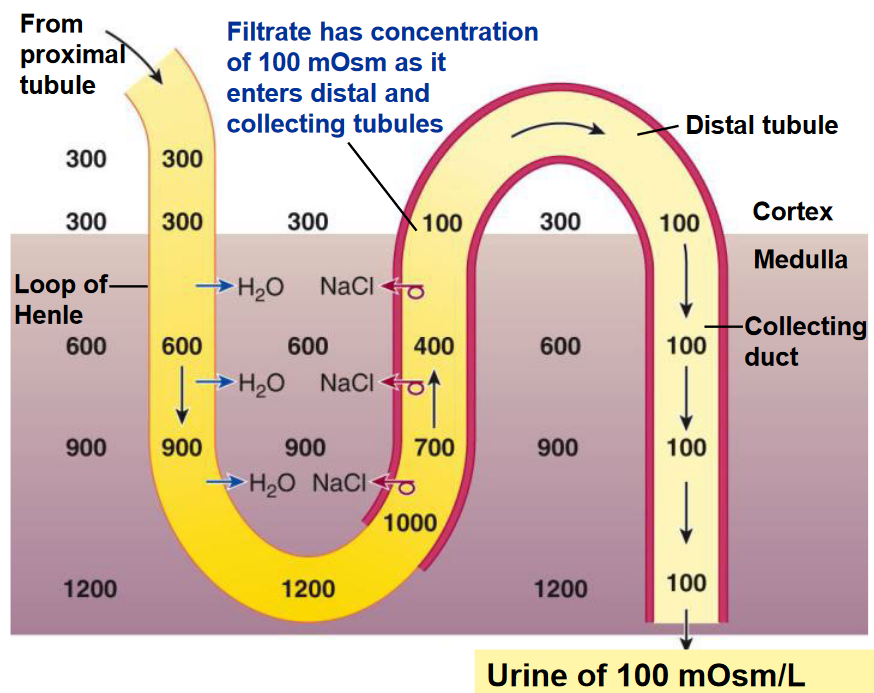
Figure 12.10: Diluted Urine in the Absence of ADH
In the presence of ADH, the kidneys begin to produce concentrated urine:
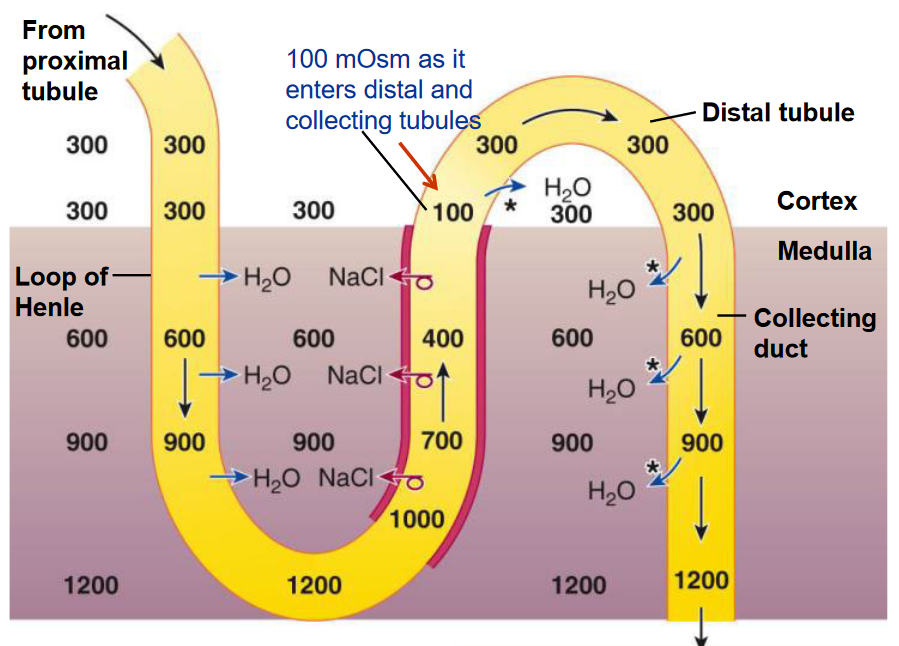
Figure 12.11: Concentrated Urine in the Presence of ADH
12.4.3 Limitations of ADH
First and foremost, ADH cannot halt urine production.
There are about 600 milliosmols of waste products and other solutes in one’s urine per day. The minimum volume needed to excrete these products and solutes is 0.5 L - under maximal ADH influence, 99.7% of the 180 L of filtered plasma is reabsorbed.
12.5 Plasma Clearance
The plasma clearance is the volume of plasma that is completely cleared of a particular substance by the kidneys per minute.
The clearance rate is:
\[\begin{equation} \frac{\text{urine concentration of substance} \times \text{urine flow rate}}{\text{plasma concentration of substance}} \end{equation}\]
12.5.1 Commonly used substances for a plasma clearance test
Insulin is a naturally-occurring protein that is freely filtered, not reabsorbed, and not secreted. The plasma clearance of Insulin is equal to the glomerular filtration rate.
Creatinine is an endogenous substance that is freely filtered, slightly secreted, and not reabsorbed. This substance is generally used for a renal function test and as a good indicator of the glomerular filtration rate and clearance.
Para-aminohippuric acid (i.e., PAH) is a synthetic substance that is freely filtered, not reabsorbed, and completely secreted. All blood that flows through the kidney is completely cleared of PAH; the plasma clearance for PAH estiamtes the renal plasma flow.
12.5.2 Consequences of renal failure
Uremia is the accumulation of waste products. Metabolic acidosis may also result.
Salt and water retention can lead to Na+ imbalances and K+ retention.
Anemia and endocrine disorders may also result - the person may also develop a disorder of mineral metabolism.
Some causes of renal failure include:
- High blood pressure and antibiotics
- Infection, toxic substances, and autoimmune responses
- Obstruction of the urinary tract (e.g., a kidney stone)
- Insufficient blood supply to the kidneys
Note that kidney (i.e., renal) failure may also occur as acute renal failure (i.e., the rapid loss of renal function) or as chronic renal failure (i.e., a progression in the disease of the kidneys, a gradual loss of renal functions, and irreversible damage).
12.5.2.1 Hemodialysis
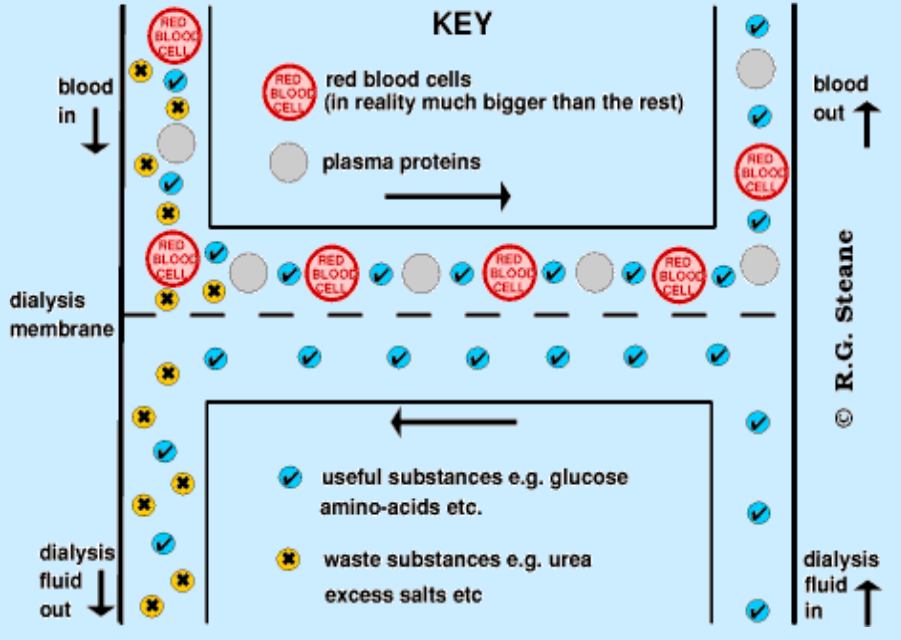
Figure 12.12: Dialysis Mechanism
A treatment for renal failure is dialysis: molecules are separated on the basis of their ability to diffuse through a selectively permeable membrane.
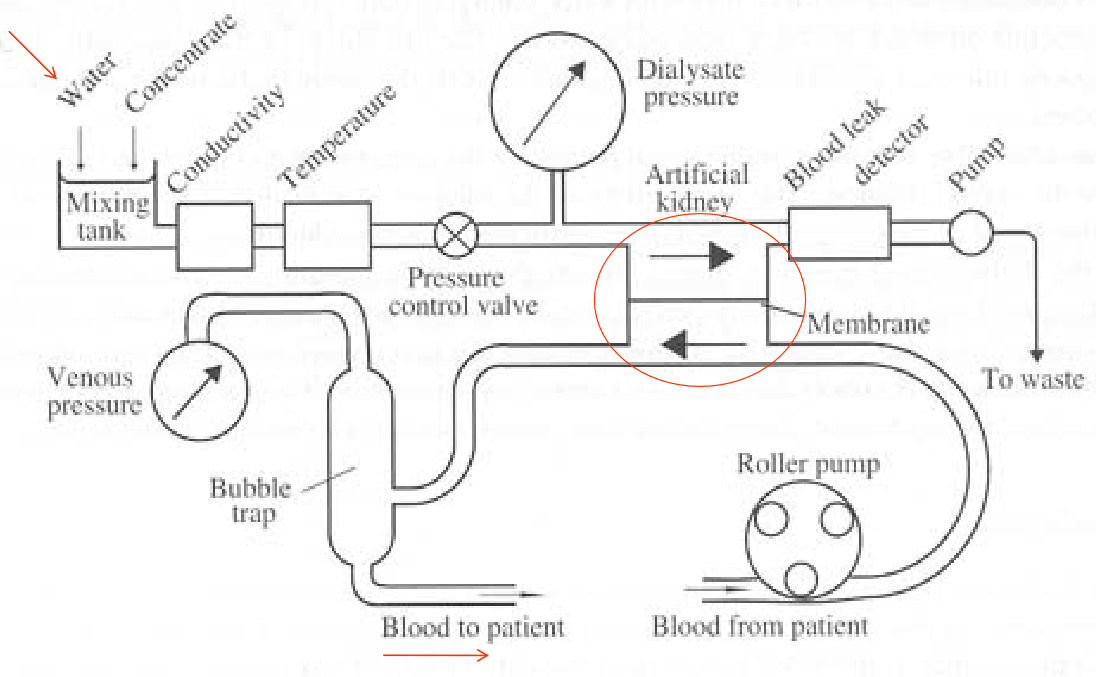
Figure 12.13: Hemodialysis Setup
Also observe the typical setup for dialysis treatments.